Chapter 3 - The Physiology of Diving and Nitrox
The Physiology of Diving and Nitrox
37
tain military and commercial diving, or recompression
chamber treatment.
Pulmonary toxicity is not a concern of the recreational
nitrox diver; CNS toxicity is a concern.
CENTRAL NERVOUS SYSTEM TOXICITY
Susceptibility to CNS oxygen toxicity varies greatly
between individuals and is affected by other factors and
conditions as well. One’s oxygen tolerance has also
been shown to vary from day to day. It is impossible to
predictably relate CNS oxygen toxicity appearance to
any definite PO2 and time exposure. Nevertheless, it is
certain that the greater the oxygen partial pressure and
the longer the time of exposure, the more likely it is
that symptoms of CNS oxygen toxicity will develop. In
setting oxygen exposure limits, it is best to err on the
side of safety.
Beginning with its first presentation of oxygen
enriched air for scuba diving in the second edition
of the NOAA Diving Manual (1979), NOAA has
recommended a maximum oxygen partial pressure
of 1.6 ata. In the new fourth edition (2001), they
add the cautionary comment: “A slightly lower level
provides less oxygen exposure risk.” Diving to a PO2
higher than 1.6 ata has been likened to knocking on
the door of a casino. Once you go in, you could win,
or you could lose a little, or you could lose a lot, but
in the long run the house always wins. For recreational
nitrox diving, the generally accepted PO2 exposure
limit is 1.4 atmospheres absolute, with 1.6 ata
reserved for contingencies. With appropriate selection
of your enriched air nitrox mixture, 1.4 ata PO2 is
more than adequate for 99.9% of the dives you may
want to accomplish.
Among the many factors that can increase your
susceptibility to CNS oxygen toxicity (an “Ox-Tox
Hit”) are heavy exercise, increased carbon dioxide
build-up from whatever cause, chilling or hypothermia,
and water immersion (as opposed to “chamber
diving”). One cannot predict oxygen toxicity.
It is also impossible to predict a reliable sequence of
toxicity signs and symptoms. The first noticeable sign
may be the epilepsy-like convulsions. This may not be
serious in itself, but it is most certainly a problem if it
occurs at a depth of 30 meters (100 feet) while breathing
out of a scuba regulator. Drowning is a very likely
result. Many preliminary manifestations of CNS oxygen
toxicity have been reported, either singly or in combination.
The mnemonic acronym “ConVENTID” is useful
for remembering the most obvious of them. ConVENTID
stands for: Convulsions, Visual disturbances, Ears,
Nausea, Twitching or Tingling, Irritability, and Dizziness
or Dyspnea.
• Convulsions are the most obvious and most
serious signs. Possible precursors to convulsions are:
• Visual disturbances, tunnel vision, dazzle or
seeing “fireflies.”
• Ear ringing, tinnitus, or sounds like an approaching
train in a tunnel.
• Nausea, including vomiting.
• Twitching, especially of the lips and small facial
muscles or the hands, or tingling (paresthesia)
especially in the fingers.
• Irritability, restlessness, euphoria, dysphoria (uneasiness
or feelings of impending doom), anxiety, or
general confusion.
• Dizziness and vertigo or dyspnea (difficult or
labored breathing).
Other signs can include facial pallor, slowed heart rate
(bradycardia), pupil dilation, hiccups, and hallucinations.
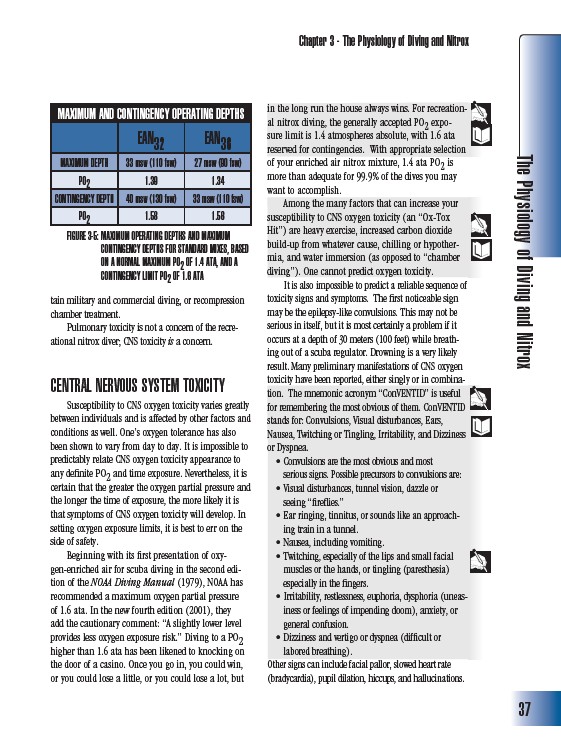
MAXIMUM AND CONTINGENCY OPERATING DEPTHS
EAN32 EAN36
MAXIMUM DEPTH 33 msw (110 fsw) 27 msw (90 fsw)
PO2 1.39 1.34
CONTINGENCY DEPTH 40 msw (130 fsw) 33 msw (110 fsw)
PO2 1.58 1.56
FIGURE 3-5: MAXIMUM OPERATING DEPTHS AND MAXIMUM
CONTINGENCY DEPTHS FOR STANDARD MIXES, BASED
ON A NORMAL MAXIMUM PO2 OF 1.4 ATA, AND A
CONTINGENCY LIMIT PO2 OF 1.6 ATA