Tear Along Dotted Line
Superior Vision Coverage
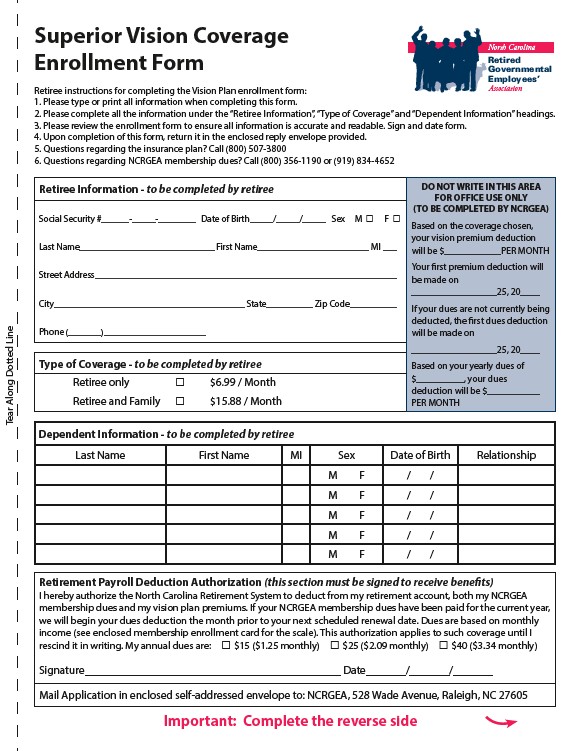
Enrollment Form
Retiree instructions for completing the Vision Plan enrollment form:
1. Please type or print all information when completing this form.
2. Please complete all the information under the “Retiree Information”, “Type of Coverage” and “Dependent Information” headings.
3. Please review the enrollment form to ensure all information is accurate and readable. Sign and date form.
4. Upon completion of this form, return it in the enclosed reply envelope provided.
5. Questions regarding the insurance plan? Call (800) 507-3800
6. Questions regarding NCRGEA membership dues? Call (800) 356-1190 or (919) 834-4652
Retiree Information - to be completed by retiree
Social Security #______-_____-________ Date of Birth_____/_____/_____ Sex M P F P
Last Name_____________________________ First Name________________________ MI ___
Street Address_________________________________________________________________
City_________________________________________ State__________ Zip Code __________
Phone (_______)______________________
Type of Coverage - to be completed by retiree
Retiree only P $6.99 / Month
Retiree and Family P $15.88 / Month
North Carolina
Retired
Governmental
Employees’
Association
DO NOT WRITE IN THIS AREA
FOR OFFICE USE ONLY
(TO BE COMPLETED BY NCRGEA)
Based on the coverage chosen,
your vision premium deduction
will be $____________PER MONTH
Your fi rst premium deduction will
be made on
__________________25, 20____
If your dues are not currently being
deducted, the fi rst dues deduction
will be made on
__________________25, 20____
Based on your yearly dues of
$__________, your dues
deduction will be $___________
PER MONTH
Dependent Information - to be completed by retiree
Last Name First Name MI Sex Date of Birth Relationship
M F / /
M F / /
M F / /
M F / /
M F / /
Retirement Payroll Deduction Authorization (this section must be signed to receive benefi ts)
I hereby authorize the North Carolina Retirement System to deduct from my retirement account, both my NCRGEA
membership dues and my vision plan premiums. If your NCRGEA membership dues have been paid for the current year,
we will begin your dues deduction the month prior to your next scheduled renewal date. Dues are based on monthly
income (see enclosed membership enrollment card for the scale). This authorization applies to such coverage until I
rescind it in writing. My annual dues are: P $15 ($1.25 monthly) P $25 ($2.09 monthly) P $40 ($3.34 monthly)
Signature_____________________________________________ Date_______/_______/_______
Mail Application in enclosed self-addressed envelope to: NCRGEA, 528 Wade Avenue, Raleigh, NC 27605
Important: Complete the reverse side