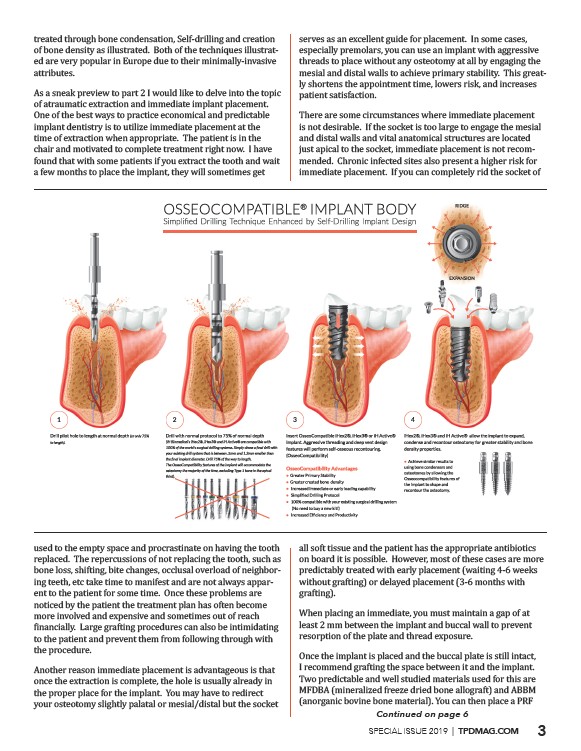
treated through bone condensation, Self-drilling and creation
of bone density as illustrated. Both of the techniques illustrated
are very popular in Europe due to their minimally-invasive
attributes.
As a sneak preview to part 2 I would like to delve into the topic
of atraumatic extraction and immediate implant placement.
One of the best ways to practice economical and predictable
implant dentistry is to utilize immediate placement at the
time of extraction when appropriate. The patient is in the
chair and motivated to complete treatment right now. I have
found that with some patients if you extract the tooth and wait
a few months to place the implant, they will sometimes get
used to the empty space and procrastinate on having the tooth
replaced. The repercussions of not replacing the tooth, such as
bone loss, shifting, bite changes, occlusal overload of neighboring
teeth, etc take time to manifest and are not always apparent
to the patient for some time. Once these problems are
noticed by the patient the treatment plan has often become
more involved and expensive and sometimes out of reach
����������������������������������������������������������������������������������������������������������������������������������
to the patient and prevent them from following through with
the procedure.
Another reason immediate placement is advantageous is that
once the extraction is complete, the hole is usually already in
the proper place for the implant. You may have to redirect
your osteotomy slightly palatal or mesial/distal but the socket
serves as an excellent guide for placement. In some cases,
especially premolars, you can use an implant with aggressive
threads to place without any osteotomy at all by engaging the
mesial and distal walls to achieve primary stability. This greatly
shortens the appointment time, lowers risk, and increases
patient satisfaction.
There are some circumstances where immediate placement
is not desirable. If the socket is too large to engage the mesial
and distal walls and vital anatomical structures are located
just apical to the socket, immediate placement is not recommended.
Chronic infected sites also present a higher risk for
immediate placement. If you can completely rid the socket of
all soft tissue and the patient has the appropriate antibiotics
on board it is possible. However, most of these cases are more
������������������������������������������������������������������������������������������������������������������������
����������������������������������������������������������������������������������������������������������������
��������������������
When placing an immediate, you must maintain a gap of at
least 2 mm between the implant and buccal wall to prevent
resorption of the plate and thread exposure.
Once the implant is placed and the buccal plate is still intact,
I recommend grafting the space between it and the implant.
Two predictable and well studied materials used for this are
������������������������������������������������������������������������������������������������������������������
����������������������������������������������������������������������������������������������������������������������
��������������������������������������������������������������������������
Continued on page 6
SPECIAL ISSUE 2019 | TPDMAG.COM 3
/TPDMAG.COM