North Carolina
Retired
Governmental
Employees’
7
Tear Along Dotted Line
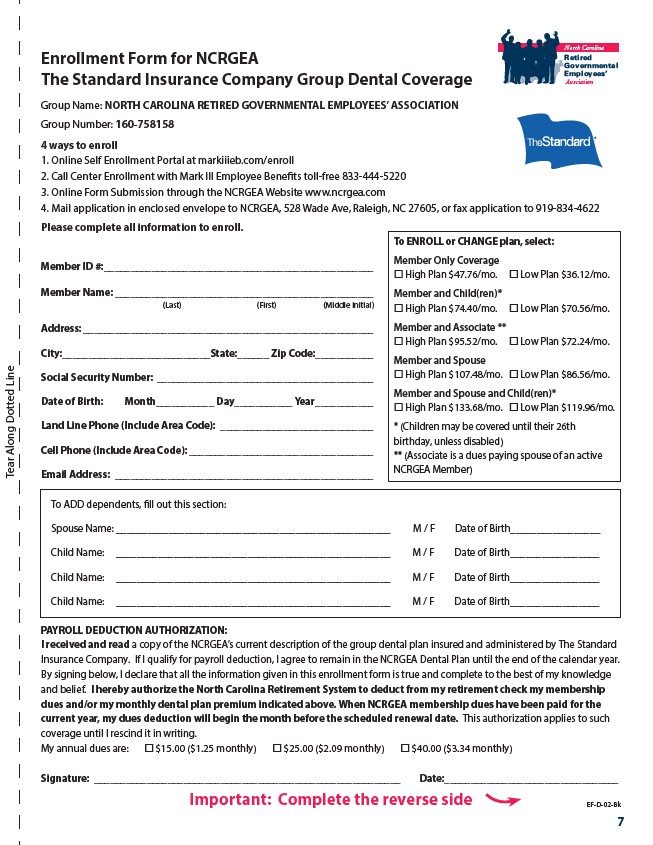
Enrollment Form for NCRGEA
The Standard Insurance Company Group Dental Coverage
Group Name: NORTH CAROLINA RETIRED GOVERNMENTAL EMPLOYEES’ ASSOCIATION
Group Number: 160-758158
4 ways to enroll
1. Online Self Enrollment Portal at markiiieb.com/enroll
2. Call Center Enrollment with Mark III Employee Benefits toll-free 833-444-5220
3. Online Form Submission through the NCRGEA Website www.ncrgea.com
4. Mail application in enclosed envelope to NCRGEA, 528 Wade Ave, Raleigh, NC 27605, or fax application to 919-834-4622
Please complete all information to enroll.
Member ID #: ___________________________________________________
Member Name: _________________________________________________
(Last) (First) (Middle Initial)
Address: _______________________________________________________
City:____________________________State:______ Zip Code: __________
Social Security Number: _________________________________________
Date of Birth: Month___________ Day___________ Year ___________
Land Line Phone (Include Area Code): _____________________________
Cell Phone (Include Area Code): ___________________________________
Email Address: _________________________________________________
Association
To ENROLL or CHANGE plan, select:
Member Only Coverage
�� High Plan $47.76/mo. �� Low Plan $36.12/mo.
Member and Child(ren)*
�� High Plan $74.40/mo. �� Low Plan $70.56/mo.
Member and Associate **
�� High Plan $95.52/mo. �� Low Plan $72.24/mo.
Member and Spouse
�� High Plan $107.48/mo. �� Low Plan $86.56/mo.
Member and Spouse and Child(ren)*
�� High Plan $133.68/mo. �� Low Plan $119.96/mo.
* (Children may be covered until their 26th
birthday, unless disabled)
** (Associate is a dues paying spouse of an active
NCRGEA Member)
To ADD dependents, fill out this section:
Spouse Name: ____________________________________________________ M / F Date of Birth_________________
Child Name: ____________________________________________________ M / F Date of Birth_________________
Child Name: ____________________________________________________ M / F Date of Birth_________________
Child Name: ____________________________________________________ M / F Date of Birth_________________
PAYROLL DEDUCTION AUTHORIZATION:
I received and read a copy of the NCRGEA’s current description of the group dental plan insured and administered by The Standard
Insurance Company. If I qualify for payroll deduction, I agree to remain in the NCRGEA Dental Plan until the end of the calendar year.
By signing below, I declare that all the information given in this enrollment form is true and complete to the best of my knowledge
and belief. I hereby authorize the North Carolina Retirement System to deduct from my retirement check my membership
dues and/or my monthly dental plan premium indicated above. When NCRGEA membership dues have been paid for the
current year, my dues deduction will begin the month before the scheduled renewal date. This authorization applies to such
coverage until I rescind it in writing.
My annual dues are: �� $15.00 ($1.25 monthly) �� $25.00 ($2.09 monthly) �� $40.00 ($3.34 monthly)
Signature: __________________________________________________________ Date:_________________________________
EF-D-02-Bk
Important: Complete the reverse side