10
VISION COVERAGE
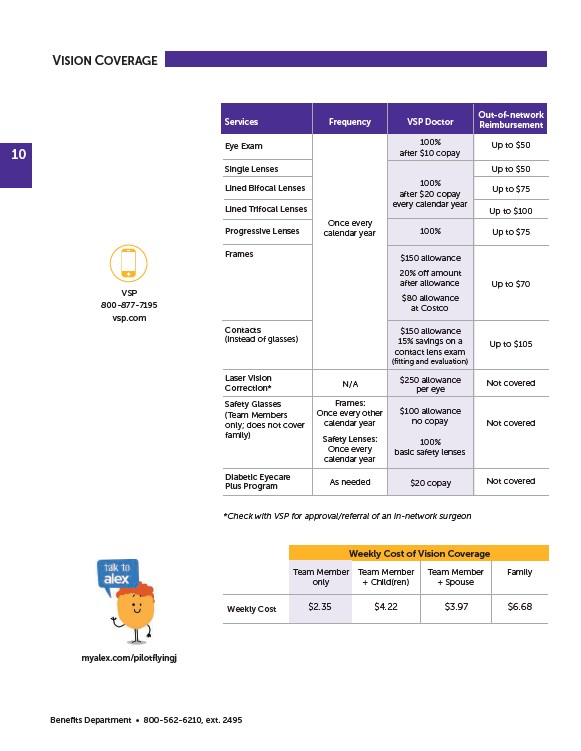
*Check with VSP for approval/referral of an in-network surgeon
Benefits Department • 800-562-6210, ext. 2495
Frequency
Once every
calendar year
N/A
Frames:
Once every other
calendar year
Safety Lenses:
Once every
calendar year
As needed
Services
Eye Exam
Single Lenses
Lined Bifocal Lenses
Lined Trifocal Lenses
Progressive Lenses
Frames
Contacts
(instead of glasses)
Laser Vision
Correction*
Safety Glasses
(Team Members
only; does not cover
family)
Diabetic Eyecare
Plus Program
VSP Doctor
100%
after $10 copay
100%
after $20 copay
every calendar year
100%
$150 allowance
20% off amount
after allowance
$80 allowance
at Costco
$150 allowance
15% savings on a
contact lens exam
(fitting and evaluation)
$250 allowance
per eye
$100 allowance
no copay
100%
basic safety lenses
$20 copay
Out-of-network
Reimbursement
Up to $50
Up to $50
Up to $75
Up to $100
Up to $75
Up to $70
Up to $105
Not covered
Not covered
Not covered
Weekly Cost
Team Member
only
Team Member
+ Child(ren)
Team Member
+ Spouse
Family
Weekly Cost of Vision Coverage
$2.35 $4.22 $3.97 $6.68
VSP
800-877-7195
vsp.com
myalex.com/pilotflyingj
/vsp.com
/pilotflyingj