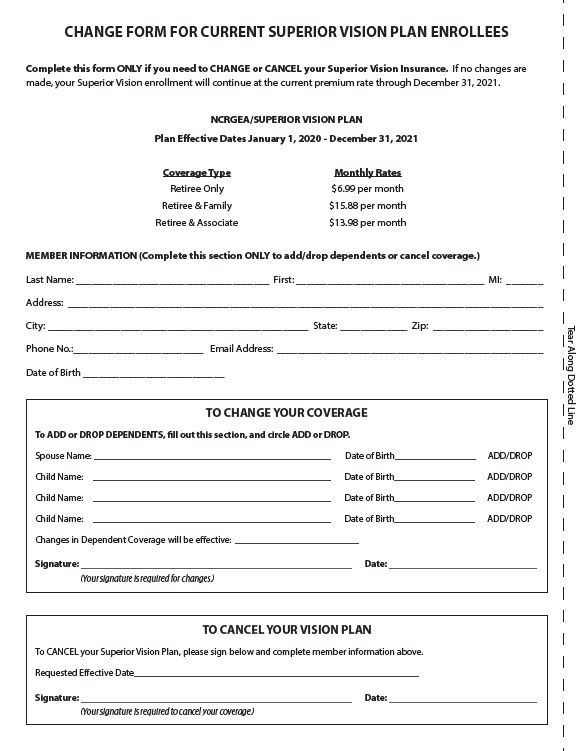
CHANGE FORM FOR CURRENT SUPERIOR VISION PLAN ENROLLEES
Complete this form ONLY if you need to CHANGE or CANCEL your Superior Vision Insurance. If no changes are
made, your Superior Vision enrollment will continue at the current premium rate through December 31, 2021.
NCRGEA/SUPERIOR VISION PLAN
Plan Effective Dates January 1, 2020 - December 31, 2021
Coverage Type Monthly Rates
Retiree Only $6.99 per month
Retiree & Family $15.88 per month
Retiree & Associate $13.98 per month
MEMBER INFORMATION (Complete this section ONLY to add/drop dependents or cancel coverage.)
Last Name: _____________________________________ First: ____________________________________ MI: _______
Address: ___________________________________________________________________________________________
City: __________________________________________________ State: _____________ Zip: _____________________
Phone No.:_________________________ Email Address: ___________________________________________________
Date of Birth ___________________________
TO CHANGE YOUR COVERAGE
To ADD or DROP DEPENDENTS, fill out this section, and circle ADD or DROP.
Spouse Name: __________________________________________________ Date of Birth_________________ ADD/DROP
Child Name: __________________________________________________ Date of Birth_________________ ADD/DROP
Child Name: __________________________________________________ Date of Birth_________________ ADD/DROP
Child Name: __________________________________________________ Date of Birth_________________ ADD/DROP
Changes in Dependent Coverage will be effective: __________________________
Signature: _________________________________________________________ Date: _______________________________
(Your signature is required for changes.)
TO CANCEL YOUR VISION PLAN
To CANCEL your Superior Vision Plan, please sign below and complete member information above.
Requested Effective Date____________________________________________________________
Signature: _________________________________________________________ Date: _______________________________
(Your signature is required to cancel your coverage.)
Tear Along Dotted Line