Enrollment and Change Form for NCRGEA
The Standard Insurance Company Group Dental Coverage
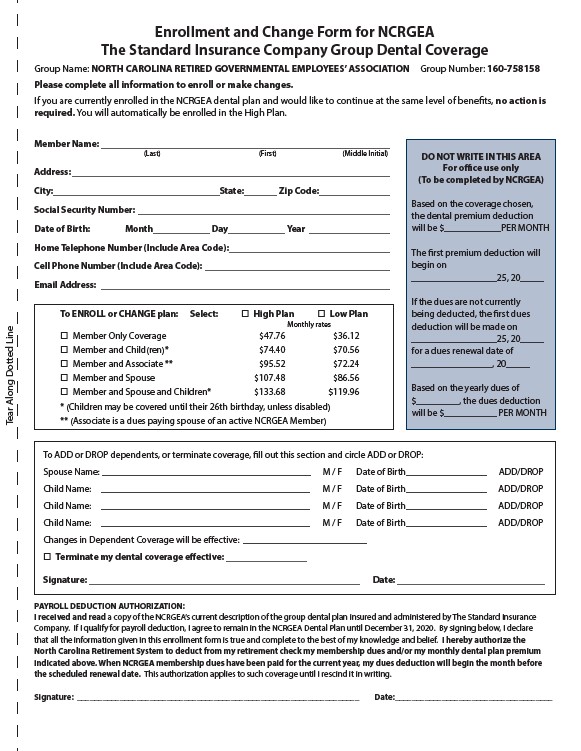
Group Name: NORTH CAROLINA RETIRED GOVERNMENTAL EMPLOYEES’ ASSOCIATION Group Number: 160-758158
Please complete all information to enroll or make changes.
If you are currently enrolled in the NCRGEA dental plan and would like to continue at the same level of benefits, no action is
required. You will automatically be enrolled in the High Plan.
Member Name: _____________________________________________________________
(Last) (First) (Middle Initial)
Address: ___________________________________________________________________
City:___________________________________State:_______ Zip Code: ______________
Social Security Number: _____________________________________________________
Date of Birth: Month____________ Day____________ Year _________________
Home Telephone Number (Include Area Code): _________________________________
Cell Phone Number (Include Area Code): _______________________________________
Email Address: _____________________________________________________________
To ENROLL or CHANGE plan: Select: �� High Plan �� Low Plan
Monthly rates
�� Member Only Coverage $47.76 $36.12
�� Member and Child(ren)* $74.40 $70.56
�� Member and Associate ** $95.52 $72.24
�� Member and Spouse $107.48 $86.56
�� Member and Spouse and Children* $133.68 $119.96
* (Children may be covered until their 26th birthday, unless disabled)
** (Associate is a dues paying spouse of an active NCRGEA Member)
DO NOT WRITE IN THIS AREA
For office use only
(To be completed by NCRGEA)
Based on the coverage chosen,
the dental premium deduction
will be $____________PER MONTH
The first premium deduction will
begin on
__________________25, 20_____
If the dues are not currently
being deducted, the first dues
deduction will be made on
__________________25, 20_____
for a dues renewal date of
_________________, 20_____
Based on the yearly dues of
$_________, the dues deduction
will be $___________ PER MONTH
To ADD or DROP dependents, or terminate coverage, fill out this section and circle ADD or DROP:
Spouse Name: ____________________________________________ M / F Date of Birth_________________ ADD/DROP
Child Name: ____________________________________________ M / F Date of Birth_________________ ADD/DROP
Child Name: ____________________________________________ M / F Date of Birth_________________ ADD/DROP
Child Name: ____________________________________________ M / F Date of Birth_________________ ADD/DROP
Changes in Dependent Coverage will be effective: __________________________
�� Terminate my dental coverage effective: _________________
Signature: _________________________________________________________ Date: _______________________________
PAYROLL DEDUCTION AUTHORIZATION:
I received and read a copy of the NCRGEA’s current description of the group dental plan insured and administered by The Standard Insurance
Company. If I qualify for payroll deduction, I agree to remain in the NCRGEA Dental Plan until December 31, 2020. By signing below, I declare
that all the information given in this enrollment form is true and complete to the best of my knowledge and belief. I hereby authorize the
North Carolina Retirement System to deduct from my retirement check my membership dues and/or my monthly dental plan premium
indicated above. When NCRGEA membership dues have been paid for the current year, my dues deduction will begin the month before
the scheduled renewal date. This authorization applies to such coverage until I rescind it in writing.
Signature: __________________________________________________________________ Date:_____________________________________
Tear Along Dotted Line