9
Health Plan
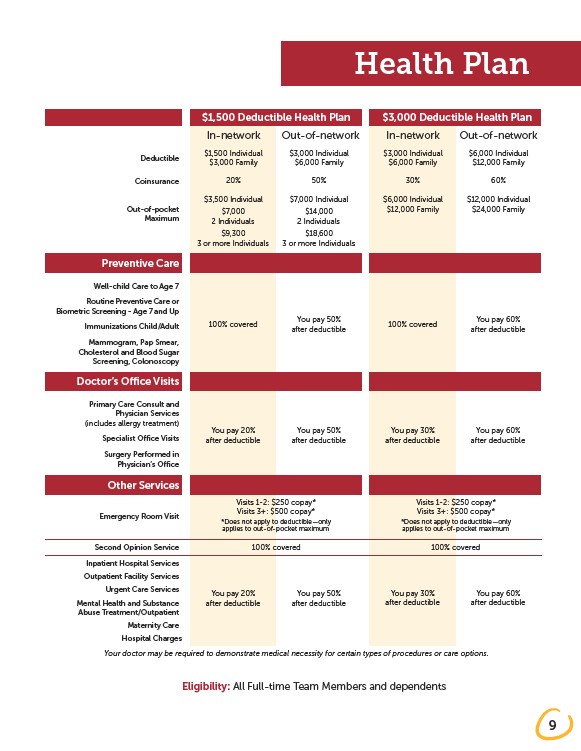
$1,500 Deductible Health Plan $3,000 Deductible Health Plan
In-network Out-of-network In-network Out-of-network
$1,500 Individual
$3,000 Family
$3,000 Individual
$6,000 Family
$3,000 Individual
$6,000 Family
$6,000 Individual
Deductible $12,000 Family
Coinsurance 20% 50% 30% 60%
$3,500 Individual
Out-of-pocket $24,000 Family
$7,000
2 Individuals
$9,300
3 or more Individuals
100% covered
$6,000 Individual
$12,000 Family
100% covered
$7,000 Individual
$14,000
2 Individuals
$18,600
3 or more Individuals
You pay 50%
after deductible
$12,000 Individual
You pay 60%
after deductible
You pay 20%
after deductible
You pay 50%
after deductible
You pay 30%
after deductible
You pay 60%
after deductible
Visits 1-2: $250 copay*
Visits 3+: $500 copay*
*Does not apply to deductible—only
applies to out-of-pocket maximum
Visits 1-2: $250 copay*
Visits 3+: $500 copay*
*Does not apply to deductible—only
applies to out-of-pocket maximum
100% covered 100% covered
You pay 20%
after deductible
You pay 50%
after deductible
You pay 30%
after deductible
You pay 60%
after deductible
Maximum
Preventive Care
Well-child Care to Age 7
Routine Preventive Care or
Biometric Screening - Age 7 and Up
Immunizations Child/Adult
Mammogram, Pap Smear,
Cholesterol and Blood Sugar
Screening, Colonoscopy
Doctor’s Office Visits
Primary Care Consult and
Physician Services
(includes allergy treatment)
Specialist Office Visits
Surgery Performed in
Physician’s Office
Other Services
Emergency Room Visit
Second Opinion Service
Inpatient Hospital Services
Outpatient Facility Services
Urgent Care Services
Mental Health and Substance
Abuse Treatment/Outpatient
Maternity Care
Hospital Charges
Your doctor may be required to demonstrate medical necessity for certain types of procedures or care options.
Eligibility: All Full-time Team Members and dependents