target can be inhibited since HIF-2a is a driver of VEGF.
If it can be blocked by using the molecule, perhaps it
could reduce the growth of lesions in various manifestations
which include eye, kidney, pancreas, brain, and
adrenal areas. The phase 1 trial generated excitement
because activity was observed in RCC and PT2977 could
produce a response in other VHL manifestations. The
clinical trial identifier is NCT03401788; EudraCT: 2018-
000125-30.
PRINCIPAL Study: Real-World Study
Captures Treatment Patterns,
Outcomes and Generates Hypotheses
Stratification by prognostic risk informs efficacy for
various treatments in patients with advanced RCC.
Whether further stratification beyond prognostic risk aids
in predicting treatment outcomes is unknown. A posthoc
analysis of real-world data, the PRINCIPAL study
(NCT01649778) assessed the effectiveness of pazopanib
in patients with intermediate risk in advanced RCC.
In this prospective, observational study, patients with
advanced and/or metastatic clear cell RCC were enrolled
within 30 days of initiating pazopanib. Data on progression,
survival, and safety were collected approximately
every 3 months until death. Primary efficacy end
points included overall survival (OS), progression-free
survival (PFS), and objective response rate (ORR). A posthoc
analysis of patients with intermediate risk per
Memorial Sloan Kettering Cancer Center (MSKCC) and
International Metastatic Renal Cell Carcinoma Database
Consortium (IMDC) criteria was conducted to evaluate
effectiveness by number or risk factors (1 vs 2), age (<65
vs �� 65 years), and Eastern Cooperative Oncology Group
performance status (ECOG PS).
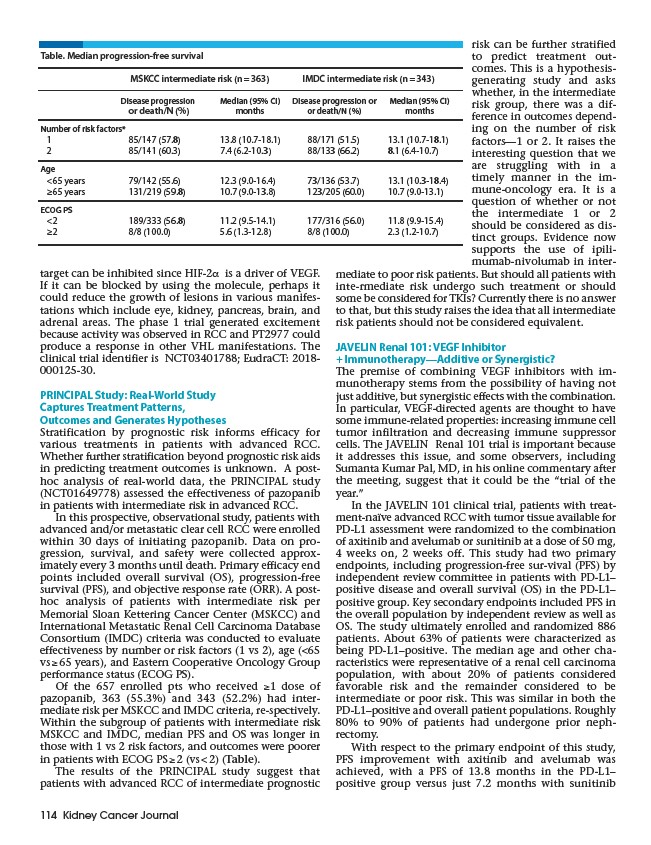
Of the 657 enrolled pts who received ��1 dose of
pazopanib, 363 (55.3%) and 343 (52.2%) had intermediate
risk per MSKCC and IMDC criteria, re-spectively.
Within the subgroup of patients with intermediate risk
MSKCC and IMDC, median PFS and OS was longer in
those with 1 vs 2 risk factors, and outcomes were poorer
in patients with ECOG PS �� 2 (vs < 2) (Table).
The results of the PRINCIPAL study suggest that
patients with advanced RCC of intermediate prognostic
114 Kidney Cancer Journal
risk can be further stratified
to predict treatment outcomes.
This is a hypothesisgenerating
study and asks
whether, in the intermediate
risk group, there was a difference
in outcomes depending
on the number of risk
factors—1 or 2. It raises the
interesting question that we
are struggling with in a
timely manner in the immune
oncology era. It is a
question of whether or not
the intermediate 1 or 2
should be considered as distinct
groups. Evidence now
supports the use of ipilimumab
nivolumab in intermediate
to poor risk patients. But should all patients with
inte-rmediate risk undergo such treatment or should
some be considered for TKIs? Currently there is no answer
to that, but this study raises the idea that all intermediate
risk patients should not be considered equivalent.
JAVELIN Renal 101: VEGF Inhibitor
+ Immunotherapy—Additive or Synergistic?
The premise of combining VEGF inhibitors with immunotherapy
stems from the possibility of having not
just additive, but synergistic effects with the combination.
In particular, VEGF-directed agents are thought to have
some immune-related properties: increasing immune cell
tumor infiltration and decreasing immune suppressor
cells. The JAVELIN Renal 101 trial is important because
it addresses this issue, and some observers, including
Sumanta Kumar Pal, MD, in his online commentary after
the meeting, suggest that it could be the “trial of the
year.”
In the JAVELIN 101 clinical trial, patients with treatment
naïve advanced RCC with tumor tissue available for
PD-L1 assessment were randomized to the combination
of axitinib and avelumab or sunitinib at a dose of 50 mg,
4 weeks on, 2 weeks off. This study had two primary
endpoints, including progression-free sur-vival (PFS) by
independent review committee in patients with PD-L1–
positive disease and overall survival (OS) in the PD-L1–
positive group. Key secondary endpoints included PFS in
the overall population by independent review as well as
OS. The study ultimately enrolled and randomized 886
patients. About 63% of patients were characterized as
being PD-L1–positive. The median age and other characteristics
were representative of a renal cell carcinoma
population, with about 20% of patients considered
favorable risk and the remainder considered to be
intermediate or poor risk. This was similar in both the
PD-L1–positive and overall patient populations. Roughly
80% to 90% of patients had undergone prior nephrectomy.
With respect to the primary endpoint of this study,
PFS improvement with axitinib and avelumab was
achieved, with a PFS of 13.8 months in the PD-L1–
positive group versus just 7.2 months with sunitinib
Table. Median progression-free survival
MSKCC intermediate risk (n = 363) IMDC intermediate risk (n = 343)
Disease progression Median (95% CI) Disease progression or Median (95% CI)
or death/N (%) months or death/N (%) months
Number of risk factors*
1 85/147 (57.8) 13.8 (10.7-18.1) 88/171 (51.5) 13.1 (10.7-18.1)
2 85/141 (60.3) 7.4 (6.2-10.3) 88/133 (66.2) 8.1 (6.4-10.7)
Age
<65 years 79/142 (55.6) 12.3 (9.0-16.4) 73/136 (53.7) 13.1 (10.3-18.4)
≥65 years 131/219 (59.8) 10.7 (9.0-13.8) 123/205 (60.0) 10.7 (9.0-13.1)
ECOG PS
<2 189/333 (56.8) 11.2 (9.5-14.1) 177/316 (56.0) 11.8 (9.9-15.4)
≥2 8/8 (100.0) 5.6 (1.3-12.8) 8/8 (100.0) 2.3 (1.2-10.7)