PROLEUKIN® (aldesleukin)
for injection, for intravenous infusion
Rx Only
WARNINGS
Therapy with Proleukin® (aldesleukin) should be restricted to patients with normal cardiac and
pulmonary functions as defined by thallium stress testing and formal pulmonary function testing.
Extreme caution should be used in patients with a normal thallium stress test and a normal pulmonary
function test who have a history of cardiac or pulmonary disease.
Proleukin should be administered in a hospital setting under the supervision of a qualified physician
experienced in the use of anticancer agents. An intensive care facility and specialists skilled in
cardiopulmonary or intensive care medicine must be available.
Proleukin administration has been associated with capillary leak syndrome (CLS) which is
characterized by a loss of vascular tone and extravasation of plasma proteins and fluid into the
extravascular space. CLS results in hypotension and reduced organ perfusion which may be
severe and can result in death. CLS may be associated with cardiac arrhythmias (supraventricular
and ventricular), angina, myocardial infarction, respiratory insufficiency requiring intubation,
gastrointestinal bleeding or infarction, renal insufficiency, edema, and mental status changes.
Proleukin treatment is associated with impaired neutrophil function (reduced chemotaxis) and with
an increased risk of disseminated infection, including sepsis and bacterial endocarditis. Consequently,
preexisting bacterial infections should be adequately treated prior to initiation of Proleukin therapy.
Patients with indwelling central lines are particularly at risk for infection with gram positive
microorganisms. Antibiotic prophylaxis with oxacillin, nafcillin, ciprofloxacin, or vancomycin has been
associated with a reduced incidence of staphylococcal infections.
Proleukin administration should be withheld in patients developing moderate to severe lethargy or
somnolence; continued administration may result in coma.
DESCRIPTION
Proleukin® (aldesleukin), a human recombinant interleukin-2 product, is a highly purified protein with a
molecular weight of approximately 15,300 daltons. The chemical name is des-alanyl-1, serine-125 human
interleukin-2. Proleukin, a lymphokine, is produced by recombinant DNA technology using a genetically
engineered E. coli strain containing an analog of the human interleukin-2 gene. Genetic engineering techniques
were used to modify the human IL-2 gene, and the resulting expression clone encodes a modified human
interleukin-2. This recombinant form differs from native interleukin-2 in the following ways: a) Proleukin is
not glycosylated because it is derived from E. coli; b) the molecule has no N-terminal alanine; the codon for
this amino acid was deleted during the genetic engineering procedure; c) the molecule has serine substituted
for cysteine at amino acid position 125; this was accomplished by site specific manipulation during the genetic
engineering procedure; and d) the aggregation state of Proleukin is likely to be different from that of native
interleukin-2.
The in vitro biological activities of the native nonrecombinant molecule have been reproduced with Proleukin.1,2
Proleukin is supplied as a sterile, white to off-white, lyophilized cake in single-use vials intended for intravenous
administration. When reconstituted with 1.2 mL Sterile Water for Injection, USP, each mL contains 18 million
International Units (1.1 mg) Proleukin, 50 mg mannitol, and 0.18 mg sodium dodecyl sulfate, buffered with
approximately 0.17 mg monobasic and 0.89 mg dibasic sodium phosphate to a pH of 7.5 (range 7.2 to 7.8).
The manufacturing process for Proleukin involves fermentation in a defined medium containing tetracycline
hydrochloride. The presence of the antibiotic is not detectable in the final product. Proleukin contains no
preservatives in the final product.
Proleukin biological potency is determined by a lymphocyte proliferation bioassay and is expressed in
International Units as established by the World Health Organization 1st International Standard for Interleukin-2
(human). The relationship between potency and protein mass is as follows:
18 million International Units Proleukin = 1.1 mg protein
CLINICAL PHARMACOLOGY
Proleukin® (aldesleukin) has been shown to possess the biological activities of human native interleukin-2.1,2 In vitro
studies performed on human cell lines demonstrate the immunoregulatory properties of Proleukin, including: a)
enhancement of lymphocyte mitogenesis and stimulation of long-term growth of human interleukin-2 dependent
cell lines; b) enhancement of lymphocyte cytotoxicity; c) induction of killer cell (lymphokine-activated (LAK) and
natural (NK)) activity; and d) induction of interferon-gamma production.
The in vivo administration of Proleukin in animals and humans produces multiple immunological effects in a dose
dependent manner. These effects include activation of cellular immunity with profound lymphocytosis, eosinophilia,
and thrombocytopenia, and the production of cytokines including tumor necrosis factor, IL-1 and gamma interferon.3
In vivo experiments in murine tumor models have shown inhibition of tumor growth.4 The exact mechanism by
which Proleukin mediates its antitumor activity in animals and humans is unknown.
Pharmacokinetics
Proleukin exists as biologically active, non-covalently bound microaggregates with an average size of 27
recombinant interleukin-2 molecules. The solubilizing agent, sodium dodecyl sulfate, may have an effect on
the kinetic properties of this product.
The pharmacokinetic profile of Proleukin is characterized by high plasma concentrations following a short
intravenous infusion, rapid distribution into the extravascular space and elimination from the body by metabolism
in the kidneys with little or no bioactive protein excreted in the urine. Studies of intravenous Proleukin in sheep and
humans indicate that upon completion of infusion, approximately 30% of the administered dose is detectable in
plasma. This finding is consistent with studies in rats using radiolabeled Proleukin, which demonstrate a rapid
(<1 min) uptake of the majority of the label into the lungs, liver, kidney, and spleen.
The serum half-life (T 1/2) curves of Proleukin remaining in the plasma are derived from studies done in 52
cancer patients following a 5-minute intravenous infusion. These patients were shown to have a distribution and
elimination T 1/2 of 13 and 85 minutes, respectively.
Following the initial rapid organ distribution, the primary route of clearance of circulating Proleukin is the kidney.
In humans and animals, Proleukin is cleared from the circulation by both glomerular filtration and peritubular
extraction in the kidney.5-8 This dual mechanism for delivery of Proleukin to the proximal tubule may account for
the preservation of clearance in patients with rising serum creatinine values. Greater than 80% of the amount of
Proleukin distributed to plasma, cleared from the circulation and presented to the kidney is metabolized to amino
acids in the cells lining the proximal convoluted tubules. In humans, the mean clearance rate in cancer patients is
268 mL/min.
The relatively rapid clearance of Proleukin has led to dosage schedules characterized by frequent, short infusions.
Observed serum levels are proportional to the dose of Proleukin.
CLINICAL STUDIES
Safety and efficacy were studied in a series of single and multicenter, historically controlled studies enrolling a total
of 525 patients with metastatic renal cell carcinoma or melanoma. Eligible patients had an Eastern Cooperative
Oncology Group (ECOG) Performance Status (PS) of 0 or 1 and normal organ function as determined by cardiac
stress test, pulmonary function tests, and creatinine ≤1.5 mg/dL. Studies excluded patients with brain metastases,
active infections, organ allografts and diseases requiring steroid treatment.
The same treatment dose and schedule was employed in all studies demonstrating efficacy. Proleukin was given by 15
min intravenous infusion every 8 hours for up to 5 days (maximum of 14 doses). No treatment was given on days 6 to 14
and then dosing was repeated for up to 5 days on days 15 to 19 (maximum of 14 doses). These 2 cycles constituted 1
course of therapy. Patients could receive a maximum of 28 doses during a course of therapy. In practice >90% of patients
had doses withheld. Doses were withheld for specific toxicities (See “DOSAGE AND ADMINISTRATION” section, “Dose
Modifications” subsection and “ADVERSE REACTIONS” section).
Metastatic Renal Cell Cancer
Two hundred fifty-five patients with metastatic renal cell cancer (metastatic RCC) were treated with single agent
Proleukin in 7 clinical studies conducted at 21 institutions. Metastatic RCC patients received a median of 20 of 28
scheduled doses of Proleukin.
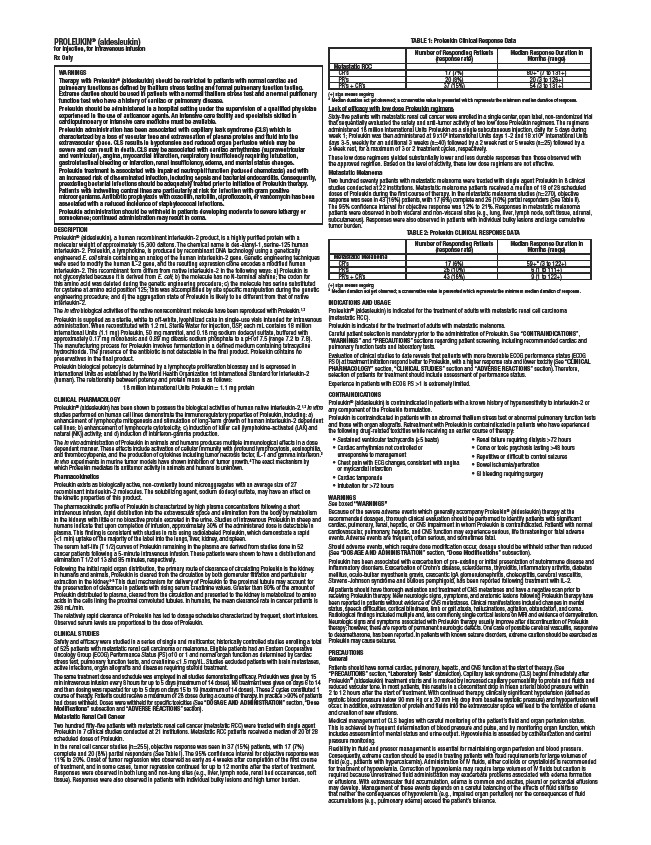
In the renal cell cancer studies (n=255), objective response was seen in 37 (15%) patients, with 17 (7%)
complete and 20 (8%) partial responders (See Table I). The 95% confidence interval for objective response was
11% to 20%. Onset of tumor regression was observed as early as 4 weeks after completion of the first course
of treatment, and in some cases, tumor regression continued for up to 12 months after the start of treatment.
Responses were observed in both lung and non-lung sites (e.g., liver, lymph node, renal bed occurrences, soft
tissue). Responses were also observed in patients with individual bulky lesions and high tumor burden.
TABLE 1: Proleukin Clinical Response Data
Number of Responding Patients
(response rate)
Median Response Duration in
Months (range)
Metastatic RCC
CR’s 17 (7%) 80+* (7 to 131+)
PR’s 20 (8%) 20 (3 to 126+)
PR’s + CR’s 37 (15%) 54 (3 to 131+)
(+) sign means ongoing
* Median duration not yet observed; a conservative value is presented which represents the minimum median duration of response.
Lack of efficacy with low dose Proleukin regimens
Sixty-five patients with metastatic renal cell cancer were enrolled in a single center, open label, non-randomized trial
that sequentially evaluated the safety and anti-tumor activity of two low dose Proleukin regimens. The regimens
administered 18 million International Units Proleukin as a single subcutaneous injection, daily for 5 days during
week 1; Proleukin was then administered at 9 x106 International Units days 1-2 and 18 x106 International Units
days 3-5, weekly for an additional 3 weeks (n=40) followed by a 2 week rest or 5 weeks (n=25) followed by a
3 week rest, for a maximum of 3 or 2 treatment cycles, respectively.
These low dose regimens yielded substantially lower and less durable responses than those observed with
the approved regimen. Based on the level of activity, these low dose regimens are not effective.
Metastatic Melanoma
Two hundred seventy patients with metastatic melanoma were treated with single agent Proleukin in 8 clinical
studies conducted at 22 institutions. Metastatic melanoma patients received a median of 18 of 28 scheduled
doses of Proleukin during the first course of therapy. In the metastatic melanoma studies (n=270), objective
response was seen in 43 (16%) patients, with 17 (6%) complete and 26 (10%) partial responders (See Table II).
The 95% confidence interval for objective response was 12% to 21%. Responses in metastatic melanoma
patients were observed in both visceral and non-visceral sites (e.g., lung, liver, lymph node, soft tissue, adrenal,
subcutaneous). Responses were also observed in patients with individual bulky lesions and large cumulative
tumor burden.
TABLE 2: Proleukin CLINICAL RESPONSE DATA
Number of Responding Patients
(response rate)
Median Response Duration in
Months (range)
Metastatic Melanoma
CR’s 17 (6%) 59+* (3 to 122+)
PR’s 26 (10%) 6 (1 to 111+)
PR’s + CR’s 43 (16%) 9 (1 to 122+)
(+) sign means ongoing
* Median duration not yet observed; a conservative value is presented which represents the minimum median duration of response.
INDICATIONS AND USAGE
Proleukin® (aldesleukin) is indicated for the treatment of adults with metastatic renal cell carcinoma
(metastatic RCC).
Proleukin is indicated for the treatment of adults with metastatic melanoma.
Careful patient selection is mandatory prior to the administration of Proleukin. See “CONTRAINDICATIONS”,
“WARNINGS” and “PRECAUTIONS” sections regarding patient screening, including recommended cardiac and
pulmonary function tests and laboratory tests.
Evaluation of clinical studies to date reveals that patients with more favorable ECOG performance status (ECOG
PS 0) at treatment initiation respond better to Proleukin, with a higher response rate and lower toxicity (See “CLINICAL
PHARMACOLOGY” section, “CLINICAL STUDIES” section and “ADVERSE REACTIONS” section). Therefore,
selection of patients for treatment should include assessment of performance status.
Experience in patients with ECOG PS >1 is extremely limited.
CONTRAINDICATIONS
Proleukin® (aldesleukin) is contraindicated in patients with a known history of hypersensitivity to interleukin-2 or
any component of the Proleukin formulation.
Proleukin is contraindicated in patients with an abnormal thallium stress test or abnormal pulmonary function tests
and those with organ allografts. Retreatment with Proleukin is contraindicated in patients who have experienced
the following drug-related toxicities while receiving an earlier course of therapy:
• Sustained ventricular tachycardia (≥5 beats)
• Cardiac arrhythmias not controlled or
• Renal failure requiring dialysis >72 hours
• Coma or toxic psychosis lasting >48 hours
• Repetitive or difficult to control seizures
• Bowel ischemia/perforation
• GI bleeding requiring surgery
unresponsive to management
• Chest pain with ECG changes, consistent with angina
or myocardial infarction
• Cardiac tamponade
• Intubation for >72 hours
WARNINGS
See boxed “WARNINGS”
Because of the severe adverse events which generally accompany Proleukin® (aldesleukin) therapy at the
recommended dosages, thorough clinical evaluation should be performed to identify patients with significant
cardiac, pulmonary, renal, hepatic, or CNS impairment in whom Proleukin is contraindicated. Patients with normal
cardiovascular, pulmonary, hepatic, and CNS function may experience serious, life threatening or fatal adverse
events. Adverse events are frequent, often serious, and sometimes fatal.
Should adverse events, which require dose modification occur, dosage should be withheld rather than reduced
(See “DOSAGE AND ADMINISTRATION” section, “Dose Modifications” subsection).
Proleukin has been associated with exacerbation of pre-existing or initial presentation of autoimmune disease and
inflammatory disorders. Exacerbation of Crohn’s disease, scleroderma, thyroiditis, inflammatory arthritis, diabetes
mellitus, oculo-bulbar myasthenia gravis, crescentic IgA glomerulonephritis, cholecystitis, cerebral vasculitis,
Stevens-Johnson syndrome and bullous pemphigoid, has been reported following treatment with IL-2.
All patients should have thorough evaluation and treatment of CNS metastases and have a negative scan prior to
receiving Proleukin therapy. New neurologic signs, symptoms, and anatomic lesions following Proleukin therapy have
been reported in patients without evidence of CNS metastases. Clinical manifestations included changes in mental
status, speech difficulties, cortical blindness, limb or gait ataxia, hallucinations, agitation, obtundation, and coma.
Radiological findings included multiple and, less commonly, single cortical lesions on MRI and evidence of demyelination.
Neurologic signs and symptoms associated with Proleukin therapy usually improve after discontinuation of Proleukin
therapy; however, there are reports of permanent neurologic defects. One case of possible cerebral vasculitis, responsive
to dexamethasone, has been reported. In patients with known seizure disorders, extreme caution should be exercised as
Proleukin may cause seizures.
PRECAUTIONS
General
Patients should have normal cardiac, pulmonary, hepatic, and CNS function at the start of therapy. (See
“PRECAUTIONS” section, “Laboratory Tests” subsection). Capillary leak syndrome (CLS) begins immediately after
Proleukin® (aldesleukin) treatment starts and is marked by increased capillary permeability to protein and fluids and
reduced vascular tone. In most patients, this results in a concomitant drop in mean arterial blood pressure within
2 to 12 hours after the start of treatment. With continued therapy, clinically significant hypotension (defined as
systolic blood pressure below 90 mm Hg or a 20 mm Hg drop from baseline systolic pressure) and hypoperfusion will
occur. In addition, extravasation of protein and fluids into the extravascular space will lead to the formation of edema
and creation of new effusions.
Medical management of CLS begins with careful monitoring of the patient’s fluid and organ perfusion status.
This is achieved by frequent determination of blood pressure and pulse, and by monitoring organ function, which
includes assessment of mental status and urine output. Hypovolemia is assessed by catheterization and central
pressure monitoring.
Flexibility in fluid and pressor management is essential for maintaining organ perfusion and blood pressure.
Consequently, extreme caution should be used in treating patients with fixed requirements for large volumes of
fluid (e.g., patients with hypercalcemia). Administration of IV fluids, either colloids or crystalloids is recommended
for treatment of hypovolemia. Correction of hypovolemia may require large volumes of IV fluids but caution is
required because unrestrained fluid administration may exacerbate problems associated with edema formation
or effusions. With extravascular fluid accumulation, edema is common and ascites, pleural or pericardial effusions
may develop. Management of these events depends on a careful balancing of the effects of fluid shifts so
that neither the consequences of hypovolemia (e.g., impaired organ perfusion) nor the consequences of fluid
accumulations (e.g., pulmonary edema) exceed the patient’s tolerance.