Clinical experience has shown that early administration of dopamine (1 to 5 mcg/kg/min) to patients manifesting
capillary leak syndrome, before the onset of hypotension, can help to maintain organ perfusion particularly to the
kidney and thus preserve urine output. Weight and urine output should be carefully monitored. If organ perfusion
and blood pressure are not sustained by dopamine therapy, clinical investigators have increased the dose of
dopamine to 6 to 10 mcg/kg/min or have added phenylephrine hydrochloride (1 to 5 mcg/kg/min) to low dose dopamine
(See “ADVERSE REACTIONS” section). Prolonged use of pressors, either in combination or as individual agents, at
relatively high doses, may be associated with cardiac rhythm disturbances. If there has been excessive weight gain
or edema formation, particularly if associated with shortness of breath from pulmonary congestion, use of
diuretics, once blood pressure has normalized, has been shown to hasten recovery. NOTE: Prior to the use of
any product mentioned, the physician should refer to the package insert for the respective product.
Proleukin® (aldesleukin) treatment should be withheld for failure to maintain organ perfusion as demonstrated by
altered mental status, reduced urine output, a fall in the systolic blood pressure below 90 mm Hg or onset of
cardiac arrhythmias (See “DOSAGE AND ADMINISTRATION” section, “Dose Modifications” subsection). Recovery
from CLS begins soon after cessation of Proleukin therapy. Usually, within a few hours, the blood pressure rises,
organ perfusion is restored and reabsorption of extravasated fluid and protein begins.
Kidney and liver function are impaired during Proleukin treatment. Use of concomitant nephrotoxic or hepatotoxic
medications may further increase toxicity to the kidney or liver.
Mental status changes including irritability, confusion, or depression which occur while receiving Proleukin may be
indicators of bacteremia or early bacterial sepsis, hypoperfusion, occult CNS malignancy, or direct Proleukininduced
CNS toxicity. Alterations in mental status due solely to Proleukin therapy may progress for several days
before recovery begins. Rarely, patients have sustained permanent neurologic deficits (See “PRECAUTIONS”
section “Drug Interactions” subsection).
Exacerbation of pre-existing autoimmune disease or initial presentation of autoimmune and inflammatory disorders
has been reported following Proleukin alone or in combination with interferon (See “PRECAUTIONS” section
“Drug Interactions” subsection and “ADVERSE REACTIONS” section). Hypothyroidism, sometimes preceded by
hyperthyroidism, has been reported following Proleukin treatment. Some of these patients required thyroid replacement
therapy. Changes in thyroid function may be a manifestation of autoimmunity. Onset of symptomatic hyperglycemia
and/or diabetes mellitus has been reported during Proleukin therapy.
Proleukin enhancement of cellular immune function may increase the risk of allograft rejection in transplant patients.
Serious Manifestations of Eosinophilia
Serious manifestations of eosinophilia involving eosinophilic infiltration of cardiac and pulmonary tissues can occur
following Proleukin.
Laboratory Tests
The following clinical evaluations are recommended for all patients, prior to beginning treatment and then daily
during drug administration.
• Standard hematologic tests-including CBC, differential and platelet counts
• Blood chemistries-including electrolytes, renal and hepatic function tests
• Chest x-rays
Serum creatinine should be ≤1.5 mg/dL prior to initiation of Proleukin treatment.
All patients should have baseline pulmonary function tests with arterial blood gases. Adequate pulmonary function
should be documented (FEV1 >2 liters or ≥75% of predicted for height and age) prior to initiating therapy.
All patients should be screened with a stress thallium study. Normal ejection fraction and unimpaired wall
motion should be documented. If a thallium stress test suggests minor wall motion abnormalities further testing
is suggested to exclude significant coronary artery disease.
Daily monitoring during therapy with Proleukin should include vital signs (temperature, pulse, blood pressure, and
respiration rate), weight, and fluid intake and output. In a patient with a decreased systolic blood pressure,
especially less than 90 mm Hg, constant cardiac rhythm monitoring should be conducted. If an abnormal complex
or rhythm is seen, an ECG should be performed. Vital signs in these hypotensive patients should be taken hourly.
During treatment, pulmonary function should be monitored on a regular basis by clinical examination,
assessment of vital signs and pulse oximetry. Patients with dyspnea or clinical signs of respiratory impairment
(tachypnea or rales) should be further assessed with arterial blood gas determination. These tests are to be
repeated as often as clinically indicated.
Cardiac function should be assessed daily by clinical examination and assessment of vital signs. Patients
with signs or symptoms of chest pain, murmurs, gallops, irregular rhythm or palpitations should be further
assessed with an ECG examination and cardiac enzyme evaluation. Evidence of myocardial injury, including
findings compatible with myocardial infarction or myocarditis, has been reported. Ventricular hypokinesia due to
myocarditis may be persistent for several months. If there is evidence of cardiac ischemia or congestive heart failure,
Proleukin therapy should be held, and a repeat thallium study should be done.
Drug Interactions
Proleukin may affect central nervous function. Therefore, interactions could occur following concomitant
administration of psychotropic drugs (e.g., narcotics, analgesics, antiemetics, sedatives, tranquilizers).
Concurrent administration of drugs possessing nephrotoxic (e.g., aminoglycosides, indomethacin), myelotoxic (e.g.,
cytotoxic chemotherapy), cardiotoxic (e.g., doxorubicin) or hepatotoxic (e.g., methotrexate, asparaginase) effects with
Proleukin may increase toxicity in these organ systems. The safety and efficacy of Proleukin in combination with any
antineoplastic agents have not been established.
In addition, reduced kidney and liver function secondary to Proleukin treatment may delay elimination of
concomitant medications and increase the risk of adverse events from those drugs.
Hypersensitivity reactions have been reported in patients receiving combination regimens containing sequential
high dose Proleukin and antineoplastic agents, specifically, dacarbazine, cis-platinum, tamoxifen and interferonalfa.
These reactions consisted of erythema, pruritus, and hypotension and occurred within hours of administration
of chemotherapy. These events required medical intervention in some patients.
Myocardial injury, including myocardial infarction, myocarditis, ventricular hypokinesia, and severe rhabdomyolysis
appear to be increased in patients receiving Proleukin and interferon-alfa concurrently.
Exacerbation or the initial presentation of a number of autoimmune and inflammatory disorders has been observed
following concurrent use of interferon-alfa and Proleukin, including crescentic IgA glomerulonephritis, oculo-bulbar
myasthenia gravis, inflammatory arthritis, thyroiditis, bullous pemphigoid, and Stevens-Johnson syndrome.
Although glucocorticoids have been shown to reduce Proleukin-induced side effects including fever, renal
insufficiency, hyperbilirubinemia, confusion, and dyspnea, concomitant administration of these agents with
Proleukin may reduce the antitumor effectiveness of Proleukin and thus should be avoided.12
Beta-blockers and other antihypertensives may potentiate the hypotension seen with Proleukin.
Delayed Adverse Reactions to Iodinated Contrast Media
A review of the literature revealed that 12.6% (range 11-28%) of 501 patients treated with various interleukin-2
containing regimens who were subsequently administered radiographic iodinated contrast media experienced acute,
atypical adverse reactions. The onset of symptoms usually occurred within hours (most commonly 1 to 4 hours)
following the administration of contrast media. These reactions include fever, chills, nausea, vomiting, pruritus,
rash, diarrhea, hypotension, edema, and oliguria. Some clinicians have noted that these reactions resemble the
immediate side effects caused by interleukin-2 administration, however the cause of contrast reactions after
interleukin-2 therapy is unknown. Most events were reported to occur when contrast media was given within
4 weeks after the last dose of interleukin-2. These events were also reported to occur when contrast media was
given several months after interleukin-2 treatment.13
Carcinogenesis, Mutagenesis, Impairment of Fertility
There have been no studies conducted assessing the carcinogenic or mutagenic potential of Proleukin.
There have been no studies conducted assessing the effect of Proleukin on fertility. It is recommended that this
drug not be administered to fertile persons of either gender not practicing effective contraception.
Pregnancy
Pregnancy Category C.
Proleukin has been shown to have embryolethal effects in rats when given in doses at 27 to 36 times the
human dose (scaled by body weight). Significant maternal toxicities were observed in pregnant rats administered
Proleukin by IV injection at doses 2.1 to 36 times higher than the human dose during critical period of
organogenesis. No evidence of teratogenicity was observed other than that attributed to maternal toxicity.
There are no adequate well-controlled studies of Proleukin in pregnant women. Proleukin should be used
during pregnancy only if the potential benefit justifies the potential risk to the fetus.
Nursing Mothers
It is not known whether this drug is excreted in human milk. Because many drugs are excreted in human milk
and because of the potential for serious adverse reactions in nursing infants from Proleukin, a decision should be
made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug
to the mother.
Pediatric Use
Safety and effectiveness in children under 18 years of age have not been established.
Geriatric Use
There were a small number of patients aged 65 and over in clinical trials of Proleukin; experience is limited to
27 patients, eight with metastatic melanoma and nineteen with metastatic renal cell carcinoma. The response
rates were similar in patients 65 years and over as compared to those less than 65 years of age. The median
number of courses and the median number of doses per course were similar between older and younger
patients.
Proleukin is known to be substantially excreted by the kidney, and the risk of toxic reactions to this drug may
be greater in patients with impaired renal function. The pattern of organ system toxicity and the proportion of
patients with severe toxicities by organ system were generally similar in patients 65 and older and younger
patients. There was a trend, however, towards an increased incidence of severe urogenital toxicities and dyspnea
in the older patients.
ADVERSE REACTIONS
The rate of drug-related deaths in the 255 metastatic RCC patients who received single-agent Proleukin®
(aldesleukin) was 4% (11/255); the rate of drug-related deaths in the 270 metastatic melanoma patients who
received single-agent Proleukin was 2% (6/270).
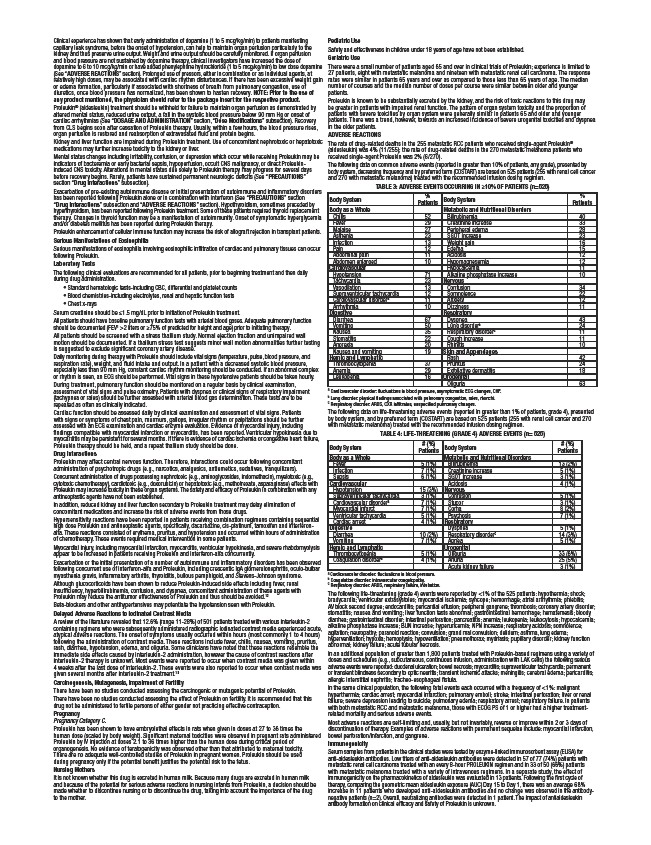
The following data on common adverse events (reported in greater than 10% of patients, any grade), presented by
body system, decreasing frequency and by preferred term (COSTART) are based on 525 patients (255 with renal cell cancer
and 270 with metastatic melanoma) treated with the recommended infusion dosing regimen.
TABLE 3: ADVERSE EVENTS OCCURRING IN ≥10% OF PATIENTS (n=525)
Body System %
Patients Body System %
Patients
Body as a Whole Metabolic and Nutritional Disorders
Chills 52 Bilirubinemia 40
Fever 29 Creatinine increase 33
Malaise 27 Peripheral edema 28
Asthenia 23 SGOT increase 23
Infection 13 Weight gain 16
Pain 12 Edema 15
Abdominal pain 11 Acidosis 12
Abdomen enlarged 10 Hypomagnesemia 12
Cardiovascular Hypocalcemia 11
Hypotension 71 Alkaline phosphatase increase 10
Tachycardia 23 Nervous
Vasodilation 13 Confusion 34
Supraventricular tachycardia 12 Somnolence 22
Cardiovascular disordera 11 Anxiety 12
Arrhythmia 10 Dizziness 11
Digestive Respiratory
Diarrhea 67 Dyspnea 43
Vomiting 50 Lung disorderb 24
Nausea 35 Respiratory disorderc 11
Stomatitis 22 Cough increase 11
Anorexia 20 Rhinitis 10
Nausea and vomiting 19 Skin and Appendages
Hemic and Lymphatic Rash 42
Thrombocytopenia 37 Pruritus 24
Anemia 29 Exfoliative dermatitis 18
Leukopenia 16 Urogenital
Oliguria 63
a Cardiovascular disorder: fluctuations in blood pressure, asymptomatic ECG changes, CHF.
b Lung disorder: physical findings associated with pulmonary congestion, rales, rhonchi.
c Respiratory disorder: ARDS, CXR infiltrates, unspecified pulmonary changes.
The following data on life-threatening adverse events (reported in greater than 1% of patients, grade 4), presented
by body system, and by preferred term (COSTART) are based on 525 patients (255 with renal cell cancer and 270
with metastatic melanoma) treated with the recommended infusion dosing regimen.
TABLE 4: LIFE-THREATENING (GRADE 4) ADVERSE EVENTS (n= 525)
Body System # (%)
Patients Body System # (%)
Patients
Body as a Whole Metabolic and Nutritional Disorders
Fever 5 (1%) Bilirubinemia 13 (2%)
Infection 7 (1%) Creatinine increase 5 (1%)
Sepsis 6 (1%) SGOT increase 3 (1%)
Cardiovascular Acidosis 4 (1%)
Hypotension 15 (3%) Nervous
Supraventricular tachycardia 3 (1%) Confusion 5 (1%)
Cardiovascular disordera 7 (1%) Stupor 3 (1%)
Myocardial infarct 7 (1%) Coma 8 (2%)
Ventricular tachycardia 5 (1%) Psychosis 7 (1%)
Cardiac arrest 4 (1%) Respiratory
Digestive Dyspnea 5 (1%)
Diarrhea 10 (2%) Respiratory disorderc 14 (3%)
Vomiting 7 (1%) Apnea 5 (1%)
Hemic and Lymphatic Urogenital
Thrombocytopenia 5 (1%) Oliguria 33 (6%)
Coagulation disorderb 4 (1%) Anuria 25 (5%)
Acute kidney failure 3 (1%)
a Cardiovascular disorder: fluctuations in blood pressure.
b Coagulation disorder: intravascular coagulopathy.
c Respiratory disorder: ARDS, respiratory failure, intubation.
The following life-threatening (grade 4) events were reported by <1% of the 525 patients: hypothermia; shock;
bradycardia; ventricular extrasystoles; myocardial ischemia; syncope; hemorrhage; atrial arrhythmia; phlebitis;
AV block second degree; endocarditis; pericardial effusion; peripheral gangrene; thrombosis; coronary artery disorder;
stomatitis; nausea and vomiting; liver function tests abnormal; gastrointestinal hemorrhage; hematemesis; bloody
diarrhea; gastrointestinal disorder; intestinal perforation; pancreatitis; anemia; leukopenia; leukocytosis; hypocalcemia;
alkaline phosphatase increase; BUN increase; hyperuricemia; NPN increase; respiratory acidosis; somnolence;
agitation; neuropathy; paranoid reaction; convulsion; grand mal convulsion; delirium; asthma, lung edema;
hyperventilation; hypoxia; hemoptysis; hypoventilation; pneumothorax; mydriasis; pupillary disorder; kidney function
abnormal; kidney failure; acute tubular necrosis.
In an additional population of greater than 1,800 patients treated with Proleukin-based regimens using a variety of
doses and schedules (e.g., subcutaneous, continuous infusion, administration with LAK cells) the following serious
adverse events were reported: duodenal ulceration; bowel necrosis; myocarditis; supraventricular tachycardia; permanent
or transient blindness secondary to optic neuritis; transient ischemic attacks; meningitis; cerebral edema; pericarditis;
allergic interstitial nephritis; tracheo-esophageal fistula.
In the same clinical population, the following fatal events each occurred with a frequency of <1%: malignant
hyperthermia; cardiac arrest; myocardial infarction; pulmonary emboli; stroke; intestinal perforation; liver or renal
failure; severe depression leading to suicide; pulmonary edema; respiratory arrest; respiratory failure. In patients
with both metastatic RCC and metastatic melanoma, those with ECOG PS of 1 or higher had a higher treatmentrelated
mortality and serious adverse events.
Most adverse reactions are self-limiting and, usually, but not invariably, reverse or improve within 2 or 3 days of
discontinuation of therapy. Examples of adverse reactions with permanent sequelae include: myocardial infarction,
bowel perforation/infarction, and gangrene.
Immunogenicity
Serum samples from patients in the clinical studies were tested by enzyme-linked immunosorbent assay (ELISA) for
anti-aldesleukin antibodies. Low titers of anti-aldesleukin antibodies were detected in 57 of 77 (74%) patients with
metastatic renal cell carcinoma treated with an every 8-hour PROLEUKIN regimen and in 33 of 50 (66%) patients
with metastatic melanoma treated with a variety of intravenous regimens. In a separate study, the effect of
immunogenicity on the pharmacokinetics of aldesleukin was evaluated in 13 patients. Following the first cycle of
therapy, comparing the geometric mean aldesleukin exposure (AUC) Day 15 to Day 1, there was an average 68%
increase in 11 patients who developed anti-aldesleukin antibodies and no change was observed in the antibodynegative
patients (n=2). Overall, neutralizing antibodies were detected in 1 patient. The impact of antialdesleukin
antibody formation on clinical efficacy and safety of Proleukin is unknown.