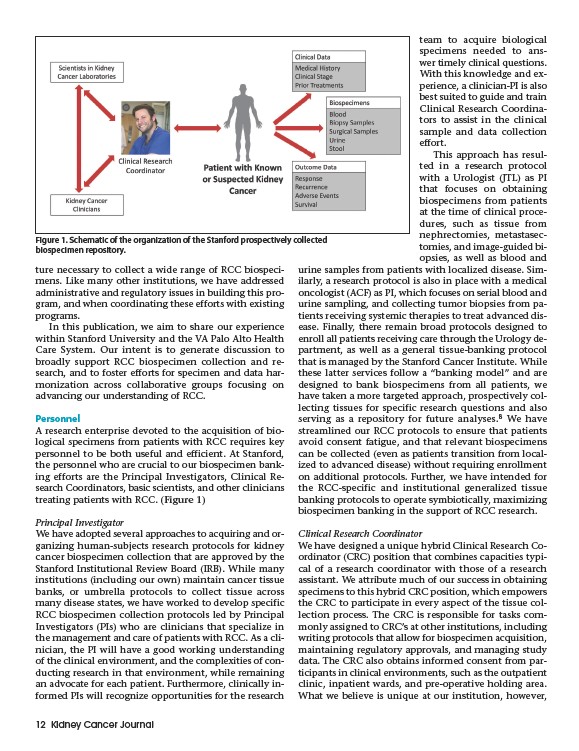
Figure 1. Schematic of the organization of the Stanford prospectively collected
biospecimen repository.
ture necessary to collect a wide range of RCC biospecimens.
Like many other institutions, we have addressed
administrative and regulatory issues in building this program,
and when coordinating these efforts with existing
programs.
In this publication, we aim to share our experience
within Stanford University and the VA Palo Alto Health
Care System. Our intent is to generate discussion to
broadly support RCC biospecimen collection and research,
and to foster efforts for specimen and data harmonization
across collaborative groups focusing on
advancing our understanding of RCC.
Personnel
A research enterprise devoted to the acquisition of biological
specimens from patients with RCC requires key
personnel to be both useful and efficient. At Stanford,
the personnel who are crucial to our biospecimen banking
efforts are the Principal Investigators, Clinical Research
Coordinators, basic scientists, and other clinicians
treating patients with RCC. (Figure 1)
Principal Investigator
We have adopted several approaches to acquiring and organizing
human-subjects research protocols for kidney
cancer biospecimen collection that are approved by the
Stanford Institutional Review Board (IRB). While many
institutions (including our own) maintain cancer tissue
banks, or umbrella protocols to collect tissue across
many disease states, we have worked to develop specific
RCC biospecimen collection protocols led by Principal
Investigators (PIs) who are clinicians that specialize in
the management and care of patients with RCC. As a clinician,
the PI will have a good working understanding
of the clinical environment, and the complexities of conducting
research in that environment, while remaining
an advocate for each patient. Furthermore, clinically informed
PIs will recognize opportunities for the research
12 Kidney Cancer Journal
team to acquire biological
specimens needed to ans-
wer timely clinical questions.
With this knowledge and experience,
a clinician-PI is also
best suited to guide and train
Clinical Research Coordinators
to assist in the clinical
sample and data collection
effort.
This approach has resulted
in a research protocol
with a Urologist (JTL) as PI
that focuses on obtaining
biospecimens from patients
at the time of clinical procedures,
such as tissue from
nephrectomies, metastasectomies,
and image-guided biopsies,
as well as blood and
urine samples from patients with localized disease. Similarly,
a research protocol is also in place with a medical
oncologist (ACF) as PI, which focuses on serial blood and
urine sampling, and collecting tumor biopsies from patients
receiving systemic therapies to treat advanced disease.
Finally, there remain broad protocols designed to
enroll all patients receiving care through the Urology department,
as well as a general tissue-banking protocol
that is managed by the Stanford Cancer Institute. While
these latter services follow a “banking model” and are
designed to bank biospecimens from all patients, we
have taken a more targeted approach, prospectively collecting
tissues for specific research questions and also
serving as a repository for future analyses.8 We have
streamlined our RCC protocols to ensure that patients
avoid consent fatigue, and that relevant biospecimens
can be collected (even as patients transition from localized
to advanced disease) without requiring enrollment
on additional protocols. Further, we have intended for
the RCC-specific and institutional generalized tissue
banking protocols to operate symbiotically, maximizing
biospecimen banking in the support of RCC research.
Clinical Research Coordinator
We have designed a unique hybrid Clinical Research Coordinator
(CRC) position that combines capacities typical
of a research coordinator with those of a research
assistant. We attribute much of our success in obtaining
specimens to this hybrid CRC position, which empowers
the CRC to participate in every aspect of the tissue collection
process. The CRC is responsible for tasks commonly
assigned to CRC’s at other institutions, including
writing protocols that allow for biospecimen acquisition,
maintaining regulatory approvals, and managing study
data. The CRC also obtains informed consent from participants
in clinical environments, such as the outpatient
clinic, inpatient wards, and pre-operative holding area.
What we believe is unique at our institution, however,