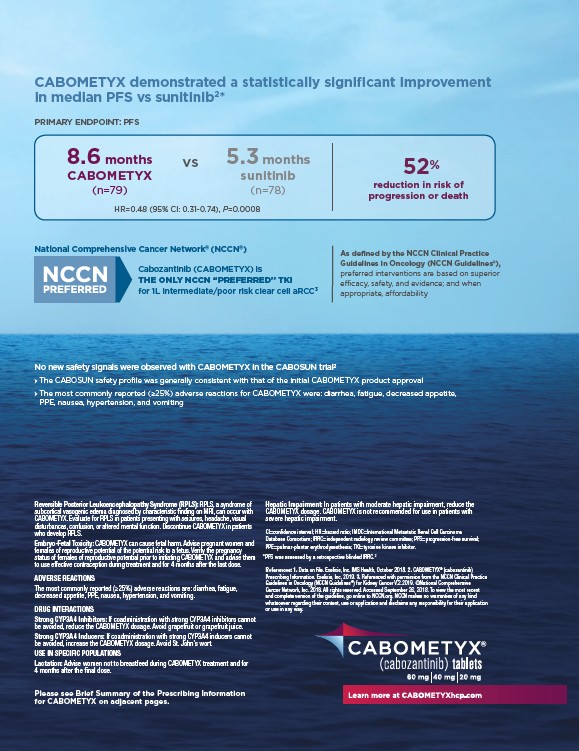
CABOMETYX demonstrated a statistically signifi cant improvement
in median PFS vs sunitinib2*
8.6 months
CABOMETYX
(n=79)
5.3 months
sunitinib
(n=78)
vs
HR=0.48 (95% CI: 0.31-0.74), P=0.0008
National Comprehensive Cancer Network® (NCCN® )
Cabozantinib (CABOMETYX) is
THE ONLY NCCN “PREFERRED” TKI
for 1L intermediate/poor risk clear cell aRCC3
Reversible Posterior Leukoencephalopathy Syndrome (RPLS): RPLS, a syndrome of
subcortical vasogenic edema diagnosed by characteristic fi nding on MRI, can occur with
CABOMETYX. Evaluate for RPLS in patients presenting with seizures, headache, visual
disturbances, confusion, or altered mental function. Discontinue CABOMETYX in patients
who develop RPLS.
Embryo-Fetal Toxicity: CABOMETYX can cause fetal harm. Advise pregnant women and
females of reproductive potential of the potential risk to a fetus. Verify the pregnancy
status of females of reproductive potential prior to initiating CABOMETYX and advise them
to use effective contraception during treatment and for 4 months after the last dose.
ADVERSE REACTIONS
The most commonly reported (≥25%) adverse reactions are: diarrhea, fatigue,
decreased appetite, PPE, nausea, hypertension, and vomiting.
DRUG INTERACTIONS
Strong CYP3A4 Inhibitors: If coadministration with strong CYP3A4 inhibitors cannot
be avoided, reduce the CABOMETYX dosage. Avoid grapefruit or grapefruit juice.
Strong CYP3A4 Inducers: If coadministration with strong CYP3A4 inducers cannot
be avoided, increase the CABOMETYX dosage. Avoid St. John’s wort.
USE IN SPECIFIC POPULATIONS
Lactation: Advise women not to breastfeed during CABOMETYX treatment and for
4 months after the fi nal dose.
52%
reduction in risk of
progression or death
As defined by the NCCN Clinical Practice
Guidelines in Oncology (NCCN Guidelines®),
preferred interventions are based on superior
efficacy, safety, and evidence; and when
appropriate, affordability
Hepatic Impairment: In patients with moderate hepatic impairment, reduce the
CABOMETYX dosage. CABOMETYX is not recommended for use in patients with
severe hepatic impairment.
CI=confi dence interval; HR=hazard ratio; IMDC=International Metastatic Renal Cell Carcinoma
Database Consortium; IRRC=independent radiology review committee; PFS=progression-free survival;
PPE=palmar-plantar erythrodysesthesia; TKI=tyrosine kinase inhibitor.
*P FS was assessed by a retrospective blinded IRRC.2
References: 1. Data on fi le. Exelixis, Inc. IMS Health, October 2018. 2. CABOMETYX® (cabozantinib)
Prescribing Information. Exelixis, Inc, 2019. 3. Referenced with permission from the NCCN Clinical Practice
Guidelines in Oncology (NCCN Guidelines®) for Kidney Cancer V.2.2019. ©National Comprehensive
Cancer Network, Inc. 2018. All rights reserved. Accessed September 26, 2018. To view the most recent
and complete version of the guideline, go online to NCCN.org. NCCN makes no warranties of any kind
whatsoever regarding their content, use or application and disclaims any responsibility for their application
or use in any way.
PRIMARY ENDPOINT: PFS
No new safety signals were observed with CABOMETYX in the CABOSUN trial2
The CABOSUN safety profi le was generally consistent with that of the initial CABOMETYX product approval
The most commonly reported (≥25%) adverse reactions for CABOMETYX were: diarrhea, fatigue, decreased appetite,
PPE, nausea, hypertension, and vomiting
Please see Brief Summary of the Prescribing Information
for CABOMETYX on adjacent pages.
/NCCN.org
/cabometyxhcp.com