Kidney Cancer Journal 79
tantly, although this trial was planned to recruit 458 patients,
poor accrual prompted its data monitoring committee
to close the trial prematurely in response to a
finding that the 28-week PFS was 42% in the immediate
CN arm (n=50) and 43% in the deferred CN arm (n=49),
a difference that was obviously not significant. However,
later report by Bex et al,2 using the same dataset, concluded
that OS was positively impacted with the deferred
CN approach because, potentially because more patients
received sunitinib. Median OS was 32.4 months in the
deferred CN arm versus 15 months in the immediate CN
arm.
Although this study’s conclusions are potentially flawed
by early termination of the study, one of the key
messages from the SURTIME trial is related to the suggestion
that patient selection for CN might be based on
early response to systemic therapy. In other words, progression
on systemic therapy, given before planned CN,
might be used to identify patients likely to be resistant
any targeted therapy and therefore unlikely to benefit
from CN. Other studies, have also have shown that presurgical
VEGFR-TKI therapy in which progressive disease
occurred in those treated with sunitinib or pazopanib before
CN was associated with shorter survival.
B
eyond SURTIME and CARMENA:
A New Algorithm to Determine the Role of CN?
As stated above, numerous studies have addressed the
implications of the SURTIME and CARMENA trials given
the fact that both trials left a trail of unanswered questions
regarding the role of CN in patients treated with sunitinib.
Subsequent papers have also attempted to
provide a useful guide directed to the appropriate selection
of candidates for CN after careful consideration
of prognostic risk factors. Updated guidelines from the
European Association of Urology and the AUA have further
clarified the role of CN.
To what extent are prognostic and predictive factors
an important part of determining survival outcomes?
Bindhi’ s review of patients with metastatic RCC16 suggested
the following:
• Poor performance status and poor IMDC/MSKCC risk
classification is associated with a poor prognosis, and
a lack of OS benefit with CN.
• Good performance status and good/intermediate
IMDC/MSKCC risk classification is predictive of OS
benefit with CN in patients without adverse IMDC/
MSKCC risk factors, who demonstrate good performance
status and low-volume metastatic burden and initial
CN generally should be considered before systemic
therapy.
• Metastectomy, when possible, markedly improves survival
and may allow patients to remain off systemic
therapy, thereby avoiding associated toxicities.
• In patients with poor IMDC/MSKCC risk disease, poor
performance status, and large-volume metastatic burden,
initial treatment with systemic therapy is generally
advised. In patients with brain metastases, spinal
metastases, and bone metastases with risk of fracture,
systemic therapy combined with radiation of the lesions
is preferred before considering CN
Future Directions: How Will Checkpoint
Inhibitors Be Integrated in the Paradigm?
One of the key issues to be addressed by planned trials is
the need to reassess the role of CN in the setting of
checkpoint inhibitor therapies that have now attained
first-line treatment status. An intriguing hypothesis is
that cytoreduction and the resultant reduction of immunosuppressive
signals may enhance the benefit of PD-L1
blockade. As trials like Checkmate-214 move forward,
the sequencing of systemic therapy and/or CN will continue
to be an essential focus of interest.
Conclusion
Although more level 1 evidence for the use of initial CN
in the era of targeted therapy is still needed, a consensus
is taking shape based on large analyses of population-
1
.75
.5
.25
0
0 20 40 60 80 100
Follow-Up (months)
Overall Survival
CN
No CN
Log rank P < .001
No. at risk
n: 8,436 1,526 391 122 32 0
n: 4,559 1,879 663 213 51 7
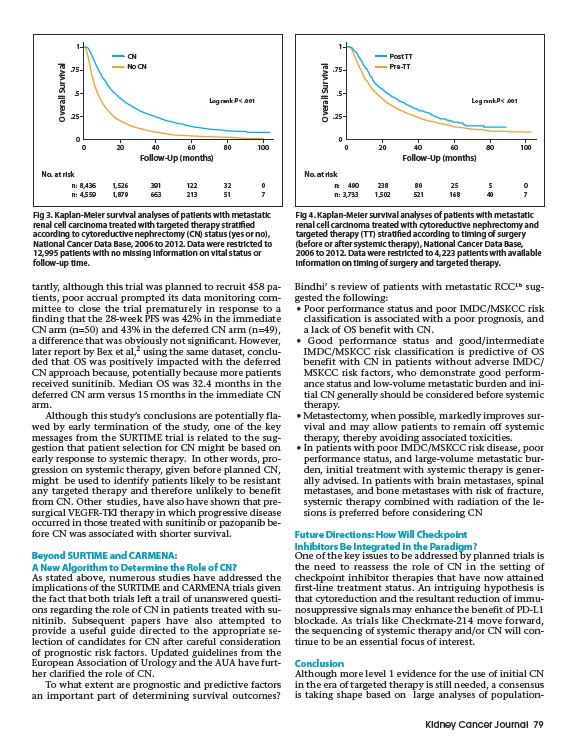
Fig 3. Kaplan-Meier survival analyses of patients with metastatic
renal cell carcinoma treated with targeted therapy stratified
according to cytoreductive nephrectomy (CN) status (yes or no),
National Cancer Data Base, 2006 to 2012. Data were restricted to
12,995 patients with no missing information on vital status or
follow-up time.
1
.75
.5
.25
0
0 20 40 60 80 100
Follow-Up (months)
Overall Survival
Post TT
Pre-TT
Log rank P < .001
No. at risk
n: 490 238 80 25 5 0
n: 3,733 1,502 521 168 40 7
Fig 4. Kaplan-Meier survival analyses of patients with metastatic
renal cell carcinoma treated with cytoreductive nephrectomy and
targeted therapy (TT) stratified according to timing of surgery
(before or after systemic therapy), National Cancer Data Base,
2006 to 2012. Data were restricted to 4,223 patients with available
information on timing of surgery and targeted therapy.