Oligometastases
asymptomatic RCC were followed with AS for a median
of 14.9 months. The key findings from the Rini report:
• A greater number of IMDC adverse risk factors and a
greater number of metastatic sites were associated
with a shorter surveillance period.
• In the favorable-prognosis group, (29 or 0% of pa-
tients) with ��1 IMDC risk factor and 2 or fewer
organs with metastatic disease, estimated median
surveillance duration was 22.2 months.
• In an unfavorable prognosis group, estimated median
surveillance duration was 8.4 months. Overall,
46% of patients died during the study from mRCC.
Although hypothesis-generating at this point, Rini et
al postulated an immunogenic basis for the good outcome
in patients who had a better prognosis with AS.
The report raises a tantalizing biologic basis for the outcomes
46 Kidney Cancer Journal
by observing that patients on AS had significantly
fewer immunosuppressive cells and a higher number of
interferon-gamma-producing T cells than the cohort of
patients who began systemic therapy immediately. If this
were true, then such a phenotype could be associated
with an anti-tumor response, perhaps accounting for the
relatively indolent nature of tumor growth reported in
patients on AS.
Following the Rini report, additional studies have further
delineated factors possibly accounting for the variation
in benefit related to AS. Two retrospective analyses
picked up on the direction from Rini et al. One of these
by Woldu et al,21 derived from 4 years of the National
Cancer Data Base, looked at the timing of targeted therapy
after cytoreductive nephrectomy—early within 2
months), moderately delayed (2- months), and delayed
(6- months). The analysis, based on data from 2716 pa-
Active
Surveillance Systemic
Rx
Local
Rx
Metastasectomy SBRT
or SBRT
Treat Observe
Continue
AS Treat
Immediate
Treatment?
Progression?
Surgically
Resectable?
NO
NO
YES
YES NO
YES NO
YES
vs
Progression?
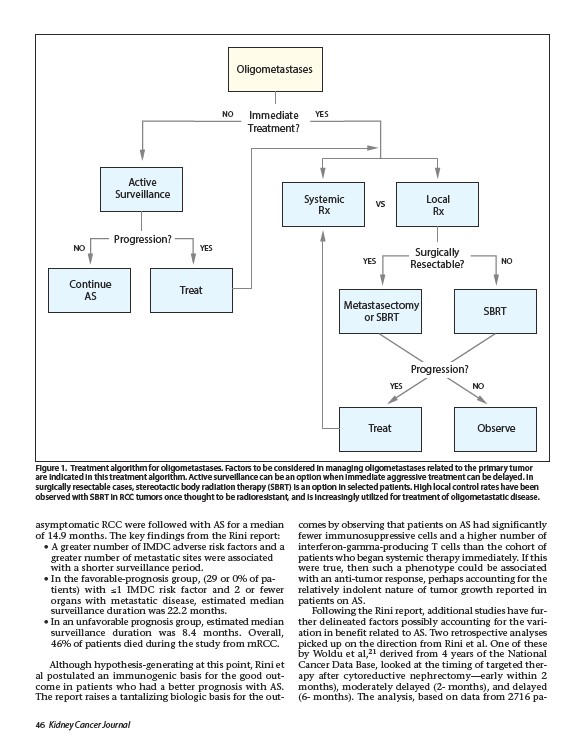
Figure 1. Treatment algorithm for oligometastases. Factors to be considered in managing oligometastases related to the primary tumor
are indicated in this treatment algorithm. Active surveillance can be an option when immediate aggressive treatment can be delayed. In
surgically resectable cases, stereotactic body radiation therapy (SBRT) is an option in selected patients. High local control rates have been
observed with SBRT in RCC tumors once thought to be radioresistant, and is increasingly utilized for treatment of oligometastatic disease.