Precision Tools for Patients with
Brain Tumors
By John Arrington, MD
Patients with brain tumors can rest assured that their
surgery or radiation treatments at Moffitt will involve
state-of-the-art tools to guide their caregivers’ hands.
To optimize surgical and radiation planning as well as
treatment of brain tumors, we post-process specialized
MRI and CT scans with Brainlab® cranial navigation
and Novalis® Radiosurgery software. This advanced
technology enables our neurosurgeons to choose the
most advantageous surgical approach for the resection
or biopsy of brain tumors. Image-guided neurosurgery
allows the neurosurgeon to visualize their surgical instruments in relation to a
patient’s brain tumor and adjacent normal brain tissue in real time during
surgery. Computer assisted neuro-surgery enables precise localization of
biopsy sites (figure) as well as allowing maximum safe resection of brain
tumors. Similar radiation planning software assists our radiation oncologists
in the planning, delivery,and monitoring of radiation therapy to brain tumors.
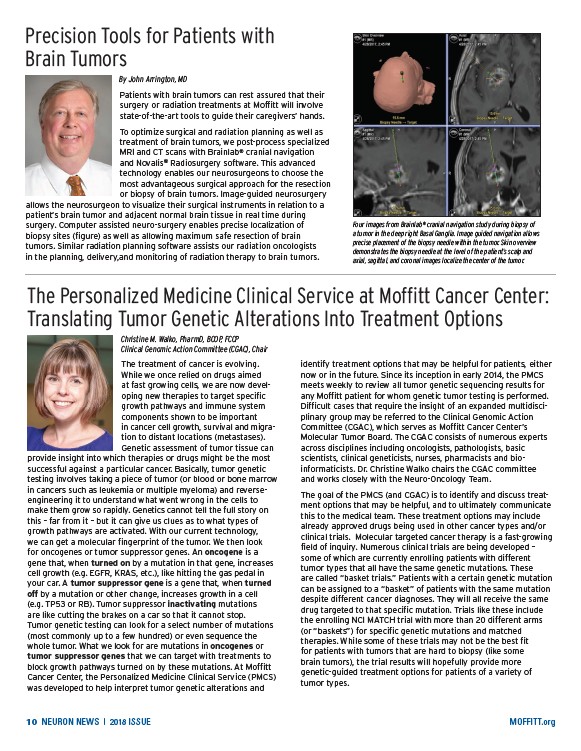
Four images from Brainlab® cranial navigation study during biopsy of
a tumor in the deep right Basal Ganglia. Image guided navigation allows
precise placement of the biopsy needle within the tumor. Skin overview
demonstrates the biopsy needle at the level of the patient’s scalp and
axial, sagittal, and coronal images localize the center of the tumor.
The Personalized Medicine Clinical Service at Moffitt Cancer Center:
Translating Tumor Genetic Alterations Into Treatment Options
Christine M. Walko, PharmD, BCOP, FCCP
Clinical Genomic Action Committee (CGAC), Chair
The treatment of cancer is evolving.
While we once relied on drugs aimed
at fast growing cells, we are now developing
new therapies to target specific
growth pathways and immune system
components shown to be important
in cancer cell growth, survival and migration
to distant locations (metastases).
Genetic assessment of tumor tissue can
provide insight into which therapies or drugs might be the most
successful against a particular cancer. Basically, tumor genetic
testing involves taking a piece of tumor (or blood or bone marrow
in cancers such as leukemia or multiple myeloma) and reverseengineering
it to understand what went wrong in the cells to
make them grow so rapidly. Genetics cannot tell the full story on
this – far from it – but it can give us clues as to what types of
growth pathways are activated. With our current technology,
we can get a molecular fingerprint of the tumor. We then look
for oncogenes or tumor suppressor genes. An oncogene is a
gene that, when turned on by a mutation in that gene, increases
cell growth (e.g. EGFR, KRAS, etc.), like hitting the gas pedal in
your car. A tumor suppressor gene is a gene that, when turned
off by a mutation or other change, increases growth in a cell
(e.g. TP53 or RB). Tumor suppressor inactivating mutations
are like cutting the brakes on a car so that it cannot stop.
Tumor genetic testing can look for a select number of mutations
(most commonly up to a few hundred) or even sequence the
whole tumor. What we look for are mutations in oncogenes or
tumor suppressor genes that we can target with treatments to
block growth pathways turned on by these mutations. At Moffitt
Cancer Center, the Personalized Medicine Clinical Service (PMCS)
was developed to help interpret tumor genetic alterations and
identify treatment options that may be helpful for patients, either
now or in the future. Since its inception in early 2014, the PMCS
meets weekly to review all tumor genetic sequencing results for
any Moffitt patient for whom genetic tumor testing is performed.
Difficult cases that require the insight of an expanded multidisciplinary
group may be referred to the Clinical Genomic Action
Committee (CGAC), which serves as Moffitt Cancer Center’s
Molecular Tumor Board. The CGAC consists of numerous experts
across disciplines including oncologists, pathologists, basic
scientists, clinical geneticists, nurses, pharmacists and bio-
informaticists. Dr. Christine Walko chairs the CGAC committee
and works closely with the Neuro-Oncology Team.
The goal of the PMCS (and CGAC) is to identify and discuss treatment
options that may be helpful, and to ultimately communicate
this to the medical team. These treatment options may include
already approved drugs being used in other cancer types and/or
clinical trials. Molecular targeted cancer therapy is a fast-growing
field of inquiry. Numerous clinical trials are being developed –
some of which are currently enrolling patients with different
tumor types that all have the same genetic mutations. These
are called “basket trials.” Patients with a certain genetic mutation
can be assigned to a “basket” of patients with the same mutation
despite different cancer diagnoses. They will all receive the same
drug targeted to that specific mutation. Trials like these include
the enrolling NCI MATCH trial with more than 20 different arms
(or “baskets”) for specific genetic mutations and matched
therapies. While some of these trials may not be the best fit
for patients with tumors that are hard to biopsy (like some
brain tumors), the trial results will hopefully provide more
genetic-guided treatment options for patients of a variety of
tumor types.
10 NEURON NEWS | 2018 ISSUE MOFFITT.org
/MOFFITT.org