Tumor Treating Fields for Glioblastoma
Nam D. Tran, MD, PhD
Glioblastoma (GBM) remains the most
common and aggressive primary brain
tumor in adults. In the US, approximately
18,000 new cases of GBM are diagnosed
every year. The gold-standard for treatment
of patients with newly diagnosed
GBM consists of maximal safe surgical
resection to the extent feasible or a
diagnostic biopsy, followed by combined
chemotherapy and radiation. Patients
then continue on maintenance chemotherapy for 6-12 months.
Clinical trials evaluating this treatment regimen have demonstrated
a median survival time of 6-7 months without evidence
of tumor growth and an overall survival of 15-16 months. Despite
improvements in delivery approaches for chemoradiation, and
surgical techniques, such as navigation-guided surgery, awake
surgeries, and functional MRI to map out critical nerve fiber
eloquent brain centers, the prognosis for GBM patients remains
dismal. There are a number of obstacles that contribute to the
poor prognosis. First, surgery can lead to damage of surrounding
brain. Chemoradiation can cause toxicity to healthy surrounding
brain tissue. And lastly, the inherent invasiveness of GBM allows
tumor cells to travel a distance away from the main tumor mass
and invade surrounding tissue. Due to this propensity to invade
and rapidly divide, tumor recurrence is almost always followed by
tumor recurrence at a focus within 1 cm of the surgical cavity.
Over the last decade all attempts and strategies to improve
outcome of patients with GBM failed when evaluated in large
randomized trials. Neither increasing the temozolomide chemotherapy
dosing, nor the addition of Avastin, the antiangiogenic
agents that disrupts blood vessel growth, nor targeting the
epidermal growth factor receptor (EGFR) with an anti-EGFR
monoclonal antibody has shown any improvement in survival.
Tumor Treating Fields (TTFields) is a
novel minimally invasive treatment
that selectively disrupts GBM tumor
cells by delivering low-intensity,
intermediate-frequency (200 kHz)
alternating electric fields via transducer
arrays applied to the scalp
(Figure 1). TTFields cause disruption
in the division process of tumor cells,
thus sending them into an apoptotic
suicide mode. In order to examine
the effectiveness of TTFields, a
multicenter, open-label, randomized
controlled phase 3 EF-14 clinical trial,
was designed to recruit 700 patients
at 90 sites in North America, Europe,
the Republic of Korea, and Israel.
Figure 1
Moffitt Cancer Center was one of the leading sites in the US,
headed by Dr. Nam Tran and the Neuro-oncology team. The trial
was designed to test the efficacy and safety of TTFields in combination
with best standard of care in the treatment of newly
diagnosed GBM. At the completion of surgery and chemoradiation,
patients were randomized to receive maintenance chemotherapy
alone or with the TTField.
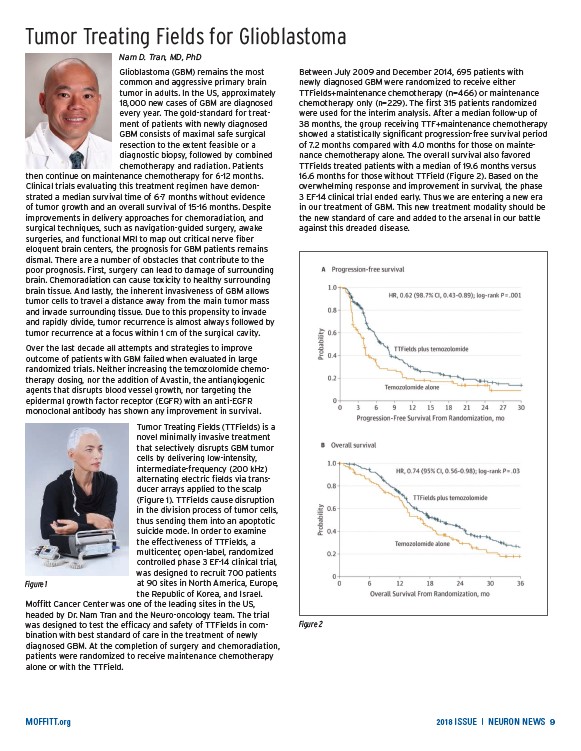
Between July 2009 and December 2014, 695 patients with
newly diagnosed GBM were randomized to receive either
TTFields+maintenance chemotherapy (n=466) or maintenance
chemotherapy only (n=229). The first 315 patients randomized
were used for the interim analysis. After a median follow-up of
38 months, the group receiving TTF+maintenance chemotherapy
showed a statistically significant progression-free survival period
of 7.2 months compared with 4.0 months for those on maintenance
TTFields treated patients with a median of 19.6 months versus
16.6 months for those without TTField (Figure 2). Based on the
overwhelming response and improvement in survival, the phase
3 EF-14 clinical trial ended early. Thus we are entering a new era
in our treatment of GBM. This new treatment modality should be
the new standard of care and added to the arsenal in our battle
against this dreaded disease.
Figure 2
chemotherapy alone. The overall survival also favored
MOFFITT.org 2018 ISSUE | NEURON NEWS 9
/MOFFITT.org