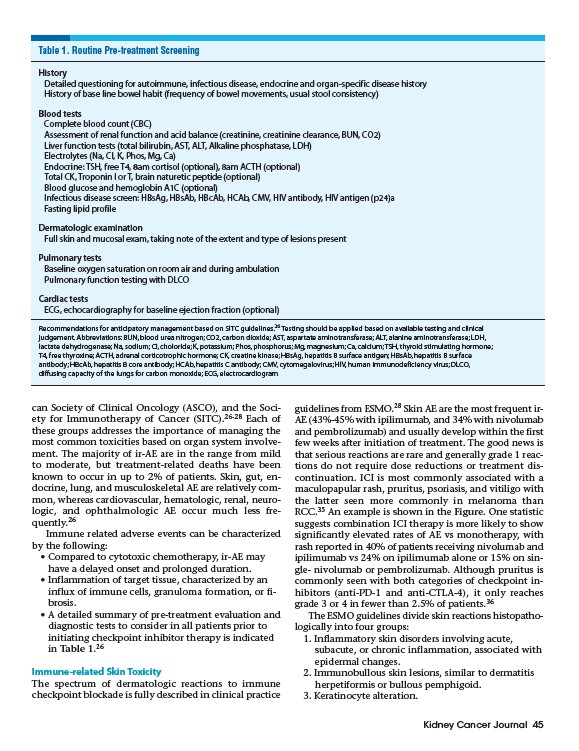
Table 1. Routine Pre-treatment Screening
History
Detailed questioning for autoimmune, infectious disease, endocrine and organ-specific disease history
History of base line bowel habit (frequency of bowel movements, usual stool consistency)
Blood tests
Complete blood count (CBC)
Assessment of renal function and acid balance (creatinine, creatinine clearance, BUN, CO2)
Liver function tests (total bilirubin, AST, ALT, Alkaline phosphatase, LDH)
Electrolytes (Na, Cl, K, Phos, Mg, Ca)
Endocrine: TSH, free T4, 8am cortisol (optional), 8am ACTH (optional)
Total CK, Troponin I or T, brain naturetic peptide (optional)
Blood glucose and hemoglobin A1C (optional)
Infectious disease screen: HBsAg, HBsAb, HBcAb, HCAb, CMV, HIV antibody, HIV antigen (p24)a
Fasting lipid profile
Dermatologic examination
Full skin and mucosal exam, taking note of the extent and type of lesions present
Pulmonary tests
Baseline oxygen saturation on room air and during ambulation
Pulmonary function testing with DLCO
Cardiac tests
ECG, echocardiography for baseline ejection fraction (optional)
Recommendations for anticipatory management based on SITC guidelines.26 Testing should be applied based on available testing and clinical
judgement. Abbreviations: BUN, blood urea nitrogen; CO2, carbon dioxide; AST, aspartate aminotransferase; ALT, alanine aminotransferase; LDH,
lactate dehydrogenase; Na, sodium; Cl, choloride; K, potassium; Phos, phosphorus; Mg, magnesium; Ca, calcium; TSH, thyroid stimulating hormone;
T4, free thyroxine; ACTH, adrenal corticotrophic hormone; CK, creatine kinase; HBsAg, hepatitis B surface antigen; HBsAb, hepatitis B surface
antibody; HBcAb, hepatitis B core antibody; HCAb, hepatitis C antibody; CMV, cytomegalovirus; HIV, human immunodeficiency virus; DLCO,
diffusing capacity of the lungs for carbon monoxide; ECG, electrocardiogram
Kidney Cancer Journal 45
can Society of Clinical Oncology (ASCO), and the Society
for Immunotherapy of Cancer (SITC).26-28 Each of
these groups addresses the importance of managing the
most common toxicities based on organ system involvement.
The majority of ir-AE are in the range from mild
to moderate, but treatment-related deaths have been
known to occur in up to 2% of patients. Skin, gut, endocrine,
lung, and musculoskeletal AE are relatively common,
whereas cardiovascular, hematologic, renal, neurologic,
and ophthalmologic AE occur much less frequently.
26
Immune related adverse events can be characterized
by the following:
• Compared to cytotoxic chemotherapy, ir-AE may
have a delayed onset and prolonged duration.
• Inflammation of target tissue, characterized by an
influx of immune cells, granuloma formation, or fibrosis.
• A detailed summary of pre-treatment evaluation and
diagnostic tests to consider in all patients prior to
initiating checkpoint inhibitor therapy is indicated
in Table 1.26
Immune-related Skin Toxicity
The spectrum of dermatologic reactions to immune
checkpoint blockade is fully described in clinical practice
guidelines from ESMO.28 Skin AE are the most frequent ir-
AE (43%-45% with ipilimumab, and 34% with nivolumab
and pembrolizumab) and usually develop within the first
few weeks after initiation of treatment. The good news is
that serious reactions are rare and generally grade 1 reactions
do not require dose reductions or treatment discontinuation.
ICI is most commonly associated with a
maculopapular rash, pruritus, psoriasis, and vitiligo with
the latter seen more commonly in melanoma than
RCC.35 An example is shown in the Figure. One statistic
suggests combination ICI therapy is more likely to show
significantly elevated rates of AE vs monotherapy, with
rash reported in 40% of patients receiving nivolumab and
ipilimumab vs 24% on ipilimumab alone or 15% on single
nivolumab or pembrolizumab. Although pruritus is
commonly seen with both categories of checkpoint inhibitors
(anti-PD-1 and anti-CTLA-4), it only reaches
grade 3 or 4 in fewer than 2.5% of patients.36
The ESMO guidelines divide skin reactions histopathologically
into four groups:
1. Inflammatory skin disorders involving acute,
subacute, or chronic inflammation, associated with
epidermal changes.
2. Immunobullous skin lesions, similar to dermatitis
herpetiformis or bullous pemphigoid.
3. Keratinocyte alteration.