Kidney Cancer Journal 47
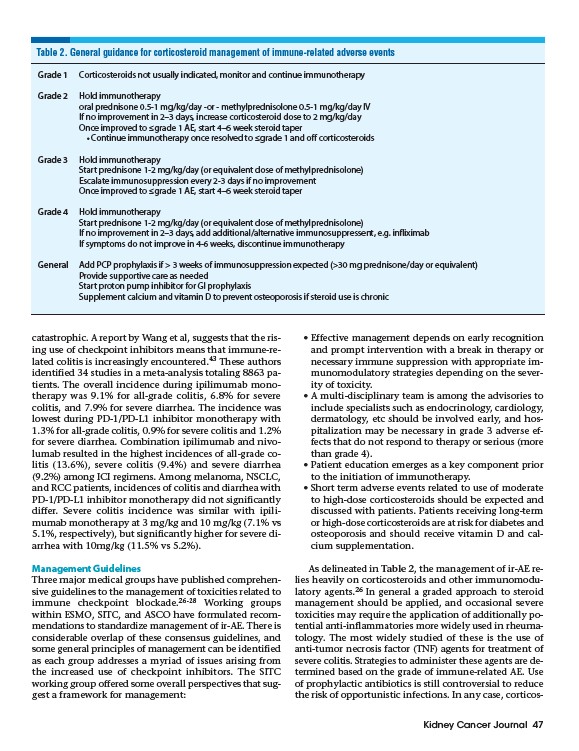
Table 2. General guidance for corticosteroid management of immune-related adverse events
Grade 1 Corticosteroids not usually indicated, monitor and continue immunotherapy
Grade 2 Hold immunotherapy
oral prednisone 0.5-1 mg/kg/day -or - methylprednisolone 0.5-1 mg/kg/day IV
If no improvement in 2–3 days, increase corticosteroid dose to 2 mg/kg/day
Once improved to ≤grade 1 AE, start 4–6 week steroid taper
• Continue immunotherapy once resolved to ≤grade 1 and off corticosteroids
catastrophic. A report by Wang et al, suggests that the rising
use of checkpoint inhibitors means that immune-related
colitis is increasingly encountered.43 These authors
identified 34 studies in a meta-analysis totaling 8863 patients.
The overall incidence during ipilimumab monotherapy
was 9.1% for all-grade colitis, 6.8% for severe
colitis, and 7.9% for severe diarrhea. The incidence was
lowest during PD-1/PD-L1 inhibitor monotherapy with
1.3% for all-grade colitis, 0.9% for severe colitis and 1.2%
for severe diarrhea. Combination ipilimumab and nivolumab
resulted in the highest incidences of all-grade colitis
(13.6%), severe colitis (9.4%) and severe diarrhea
(9.2%) among ICI regimens. Among melanoma, NSCLC,
and RCC patients, incidences of colitis and diarrhea with
PD-1/PD-L1 inhibitor monotherapy did not significantly
differ. Severe colitis incidence was similar with ipilimumab
monotherapy at 3 mg/kg and 10 mg/kg (7.1% vs
5.1%, respectively), but significantly higher for severe diarrhea
with 10mg/kg (11.5% vs 5.2%).
Management Guidelines
Three major medical groups have published comprehensive
guidelines to the management of toxicities related to
immune checkpoint blockade.26-28 Working groups
within ESMO, SITC, and ASCO have formulated recommendations
to standardize management of ir-AE. There is
considerable overlap of these consensus guidelines, and
some general principles of management can be identified
as each group addresses a myriad of issues arising from
the increased use of checkpoint inhibitors. The SITC
working group offered some overall perspectives that suggest
a framework for management:
• Effective management depends on early recognition
and prompt intervention with a break in therapy or
necessary immune suppression with appropriate immunomodulatory
strategies depending on the severity
of toxicity.
• A multi-disciplinary team is among the advisories to
include specialists such as endocrinology, cardiology,
dermatology, etc should be involved early, and hospitalization
may be necessary in grade 3 adverse effects
that do not respond to therapy or serious (more
than grade 4).
• Patient education emerges as a key component prior
to the initiation of immunotherapy.
• Short term adverse events related to use of moderate
to high-dose corticosteroids should be expected and
discussed with patients. Patients receiving long-term
or high-dose corticosteroids are at risk for diabetes and
osteoporosis and should receive vitamin D and calcium
supplementation.
As delineated in Table 2, the management of ir-AE relies
heavily on corticosteroids and other immunomodulatory
agents.26 In general a graded approach to steroid
management should be applied, and occasional severe
toxicities may require the application of additionally potential
anti-inflammatories more widely used in rheumatology.
The most widely studied of these is the use of
anti-tumor necrosis factor (TNF) agents for treatment of
severe colitis. Strategies to administer these agents are determined
based on the grade of immune-related AE. Use
of prophylactic antibiotics is still controversial to reduce
the risk of opportunistic infections. In any case, corticos-
Grade 3 Hold immunotherapy
Start prednisone 1-2 mg/kg/day (or equivalent dose of methylprednisolone)
Escalate immunosuppression every 2-3 days if no improvement
Once improved to ≤grade 1 AE, start 4–6 week steroid taper
Grade 4 Hold immunotherapy
Start prednisone 1-2 mg/kg/day (or equivalent dose of methylprednisolone)
If no improvement in 2–3 days, add additional/alternative immunosuppressent, e.g. infliximab
If symptoms do not improve in 4-6 weeks, discontinue immunotherapy
General Add PCP prophylaxis if > 3 weeks of immunosuppression expected (>30 mg prednisone/day or equivalent)
Provide supportive care as needed
Start proton pump inhibitor for GI prophylaxis
Supplement calcium and vitamin D to prevent osteoporosis if steroid use is chronic