Kidney Cancer Journal 59
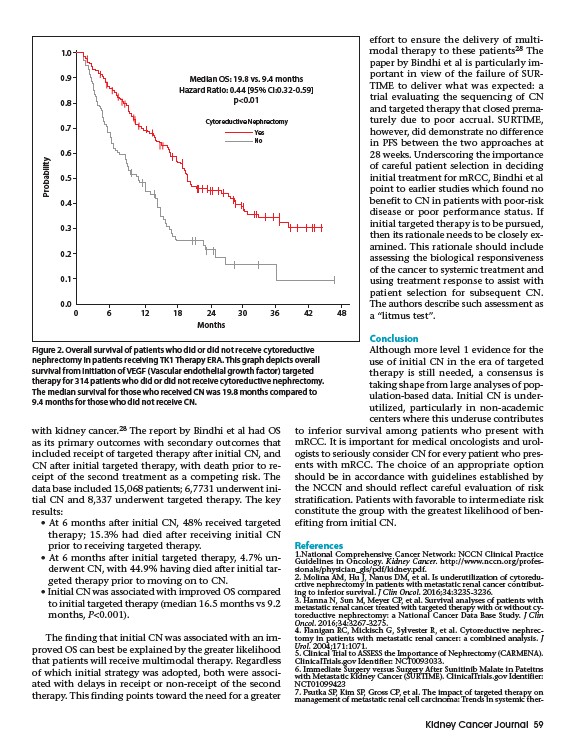
Median OS: 19.8 vs. 9.4 months
Hazard Ratio: 0.44 95% CI:0.32-0.59
with kidney cancer.28 The report by Bindhi et al had OS
as its primary outcomes with secondary outcomes that
included receipt of targeted therapy after initial CN, and
CN after initial targeted therapy, with death prior to receipt
of the second treatment as a competing risk. The
data base included 15,068 patients; 6,7731 underwent initial
CN and 8,337 underwent targeted therapy. The key
results:
• At 6 months after initial CN, 48% received targeted
therapy; 15.3% had died after receiving initial CN
prior to receiving targeted therapy.
• At 6 months after initial targeted therapy, 4.7% underwent
CN, with 44.9% having died after initial targeted
therapy prior to moving on to CN.
• Initial CN was associated with improved OS compared
to initial targeted therapy (median 16.5 months vs 9.2
months, P<0.001).
The finding that initial CN was associated with an improved
OS can best be explained by the greater likelihood
that patients will receive multimodal therapy. Regardless
of which initial strategy was adopted, both were associated
with delays in receipt or non-receipt of the second
therapy. This finding points toward the need for a greater
effort to ensure the delivery of multimodal
therapy to these patients28 The
paper by Bindhi et al is particularly important
in view of the failure of SURTIME
to deliver what was expected: a
trial evaluating the sequencing of CN
and targeted therapy that closed prematurely
due to poor accrual. SURTIME,
however, did demonstrate no difference
in PFS between the two approaches at
28 weeks. Underscoring the importance
of careful patient selection in deciding
initial treatment for mRCC, Bindhi et al
point to earlier studies which found no
benefit to CN in patients with poor-risk
disease or poor performance status. If
initial targeted therapy is to be pursued,
then its rationale needs to be closely examined.
This rationale should include
assessing the biological responsiveness
of the cancer to systemic treatment and
using treatment response to assist with
patient selection for subsequent CN.
The authors describe such assessment as
a “litmus test”.
Conclusion
Although more level 1 evidence for the
use of initial CN in the era of targeted
therapy is still needed, a consensus is
taking shape from large analyses of population
based data. Initial CN is underutilized,
particularly in non-academic
centers where this underuse contributes
to inferior survival among patients who present with
mRCC. It is important for medical oncologists and urologists
to seriously consider CN for every patient who presents
with mRCC. The choice of an appropriate option
should be in accordance with guidelines established by
the NCCN and should reflect careful evaluation of risk
stratification. Patients with favorable to intermediate risk
constitute the group with the greatest likelihood of benefiting
from initial CN.
References
1.National Comprehensive Cancer Network: NCCN Clinical Practice
Guidelines in Oncology. Kidney Cancer. http://www.nccn.org/professionals/
physician_gls/pdf/kidney.pdf.
2. Molina AM, Hu J, Nanus DM, et al. Is underutilization of cytoreducrtive
nephrectomy in patients with metastatic renal cancer contributing
to inferior survival. J Clin Oncol. 2016;34:3235-3236.
3. Hanna N, Sun M, Meyer CP, et al. Survival analyses of patients with
metastatic renal cancer treated with targeted therapy with or without cytoreductive
nephrectomy: a National Cancer Data Base Study. J Clin
Oncol. 2016;34:3267-3275.
4. Flanigan RC, Mickisch G, Sylvester R, et al. Cytoreductive nephrectomy
in patients with metastatic renal cancer: a combined analysis. J
Urol. 2004;171:1071.
5. Clinical Trial to ASSESS the Importance of Nephrectomy (CARMENA).
ClinicalTrials.gov Identifier: NCT0093033.
6. Immediate Surgery versus Surgery After Sunitinib Malate in Pateitns
with Metastatic Kidney Cancer (SURTIME). ClinicalTrials.gov Identifier:
NCT01099423
7. Psutka SP, Kim SP, Gross CP, et al. The impact of targeted therapy on
management of metastatic renal cell carcinoma: Trends in systemic ther-
6 12 18 24
Months
p<0.01
Probability
0 30 36 42 48
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
Cytoreductive Nephrectomy
Yes
No
Figure 2. Overall survival of patients who did or did not receive cytoreductive
nephrectomy in patients receiving TK1 Therapy ERA. This graph depicts overall
survival from initiation of VEGF (Vascular endothelial growth factor) targeted
therapy for 314 patients who did or did not receive cytoreductive nephrectomy.
The median survival for those who received CN was 19.8 months compared to
9.4 months for those who did not receive CN.
/ClinicalTrials.gov
/ClinicalTrials.gov