70 I ICT TODAY
When an operating room is simulated, the space will
be fitted out like an actual operating room with overhead
booms, clocks and elapsed timers. Overhead service columns
might be used to provide data to the center of the
room. For an ICU simulation space, headwalls are often
used to provide simulated services, such as vacuum and
medical gases. Often, simulated monitors are located
on or adjacent to the headwall.
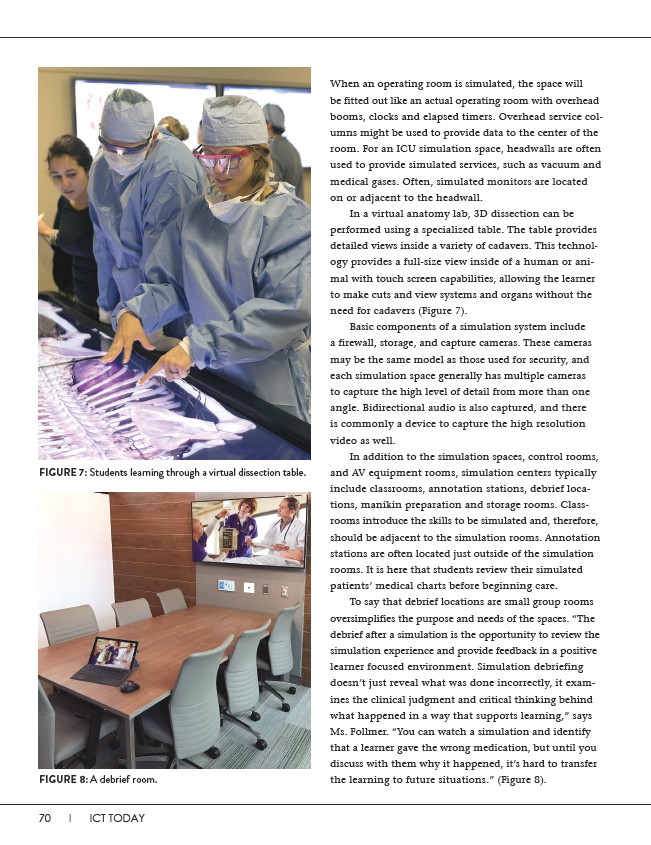
In a virtual anatomy lab, 3D dissection can be
performed using a specialized table. The table provides
detailed views inside a variety of cadavers. This technology
provides a full-size view inside of a human or animal
with touch screen capabilities, allowing the learner
to make cuts and view systems and organs without the
need for cadavers (Figure 7).
Basic components of a simulation system include
a firewall, storage, and capture cameras. These cameras
may be the same model as those used for security, and
each simulation space generally has multiple cameras
to capture the high level of detail from more than one
angle. Bidirectional audio is also captured, and there
is commonly a device to capture the high resolution
video as well.
In addition to the simulation spaces, control rooms,
and AV equipment rooms, simulation centers typically
include classrooms, annotation stations, debrief locations,
manikin preparation and storage rooms. Classrooms
introduce the skills to be simulated and, therefore,
should be adjacent to the simulation rooms. Annotation
stations are often located just outside of the simulation
rooms. It is here that students review their simulated
patients’ medical charts before beginning care.
To say that debrief locations are small group rooms
oversimplifies the purpose and needs of the spaces. “The
debrief after a simulation is the opportunity to review the
simulation experience and provide feedback in a positive
learner focused environment. Simulation debriefing
doesn’t just reveal what was done incorrectly, it examines
the clinical judgment and critical thinking behind
what happened in a way that supports learning,” says
Ms. Follmer. “You can watch a simulation and identify
that a learner gave the wrong medication, but until you
discuss with them why it happened, it’s hard to transfer
the learning to future situations.” (Figure 8).
FIGURE 7: Students learning through a virtual dissection table.
FIGURE 8: A debrief room.