Kidney Cancer Journal 13
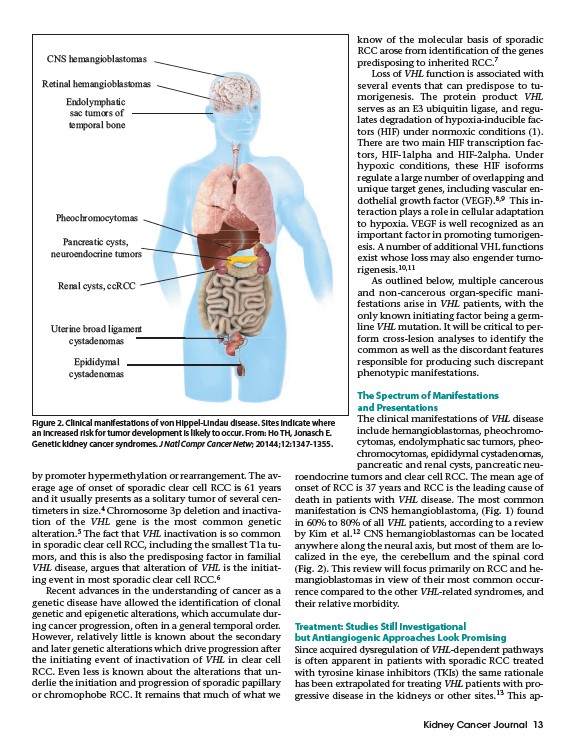
CNS hemangioblastomas
Retinal hemangioblastomas
Endolymphatic
sac tumors of
temporal bone
Pheochromocytomas
Pancreatic cysts,
neuroendocrine tumors
Renal cysts, ccRCC
Uterine broad ligament
cystadenomas
by promoter hypermethylation or rearrangement. The average
age of onset of sporadic clear cell RCC is 61 years
and it usually presents as a solitary tumor of several centimeters
in size.4 Chromosome 3p deletion and inactivation
of the VHL gene is the most common genetic
alteration.5 The fact that VHL inactivation is so common
in sporadic clear cell RCC, including the smallest T1a tumors,
and this is also the predisposing factor in familial
VHL disease, argues that alteration of VHL is the initiating
event in most sporadic clear cell RCC.6
Recent advances in the understanding of cancer as a
genetic disease have allowed the identification of clonal
genetic and epigenetic alterations, which accumulate during
cancer progression, often in a general temporal order.
However, relatively little is known about the secondary
and later genetic alterations which drive progression after
the initiating event of inactivation of VHL in clear cell
RCC. Even less is known about the alterations that underlie
the initiation and progression of sporadic papillary
or chromophobe RCC. It remains that much of what we
know of the molecular basis of sporadic
RCC arose from identification of the genes
predisposing to inherited RCC.7
Loss of VHL function is associated with
several events that can predispose to tumorigenesis.
The protein product VHL
serves as an E3 ubiquitin ligase, and regulates
degradation of hypoxia-inducible factors
(HIF) under normoxic conditions (1).
There are two main HIF transcription factors,
HIF-1alpha and HIF-2alpha. Under
hypoxic conditions, these HIF isoforms
regulate a large number of overlapping and
unique target genes, including vascular endothelial
growth factor (VEGF).8,9 This interaction
plays a role in cellular adaptation
to hypoxia. VEGF is well recognized as an
important factor in promoting tumorigenesis.
A number of additional VHL functions
exist whose loss may also engender tumorigenesis.
10,11
As outlined below, multiple cancerous
and non-cancerous organ-specific manifestations
arise in VHL patients, with the
only known initiating factor being a germline
VHL mutation. It will be critical to perform
cross-lesion analyses to identify the
common as well as the discordant features
responsible for producing such discrepant
phenotypic manifestations.
The Spectrum of Manifestations
and Presentations
The clinical manifestations of VHL disease
include hemangioblastomas, pheochromocytomas,
endolymphatic sac tumors, pheochromocytomas,
epididymal cystadenomas,
pancreatic and renal cysts, pancreatic neuroendocrine
tumors and clear cell RCC. The mean age of
onset of RCC is 37 years and RCC is the leading cause of
death in patients with VHL disease. The most common
manifestation is CNS hemangioblastoma, (Fig. 1) found
in 60% to 80% of all VHL patients, according to a review
by Kim et al.12 CNS hemangioblastomas can be located
anywhere along the neural axis, but most of them are localized
in the eye, the cerebellum and the spinal cord
(Fig. 2). This review will focus primarily on RCC and hemangioblastomas
in view of their most common occurrence
compared to the other VHL-related syndromes, and
their relative morbidity.
Treatment: Studies Still Investigational
but Antiangiogenic Approaches Look Promising
Since acquired dysregulation of VHL-dependent pathways
is often apparent in patients with sporadic RCC treated
with tyrosine kinase inhibitors (TKIs) the same rationale
has been extrapolated for treating VHL patients with progressive
disease in the kidneys or other sites.13 This ap-
Epididymal
cystadenomas
Figure 2. Clinical manifestations of von Hippel-Lindau disease. Sites indicate where
an increased risk for tumor development is likely to occur. From: Ho TH, Jonasch E.
Genetic kidney cancer syndromes. J Natl Compr Cancer Netw; 20144;12:1347-1355.