regulator and repressor of cyclin D1 transcription.25
Medullary RCC can also be differentiated from collecting
duct RCC by the presence of OCT3/4 protein on immunohistochemistry.
24,26
Translocation associated RCC are classified on the
basis of the chromosome involved (X or 6). The translocation
involves fusion of the TFE3 transcription gene with
ASPL or PRCC, configuring a distinctive RCC subtype.27
Most Xp11.2 translocation RCCs occur in pediatric populations
however in adults, it presents at an advanced
stage and displays an aggressive clinical behavior.28
Unclassified RCC represents 5% of non-clear cell RCC.
RCC tumors that do not fit other genetic and histopathologic
classifications would be categorized as unclassified
RCC. Unclassified renal cell carcinoma, which includes
tumors that are 100% sarcomatoid in appearance and for
which a more definitive tumor histology cannot be assigned,
is associated with distinct and highly aggressive
biological behavior, and poor clinical outcome. In a single
institution study, compared to clear cell carcinoma,
patients with unclassified RCC had more metastatic disease
at diagnosis, larger tumors, increased risk of adrenal
20 Kidney Cancer Journal
gland involvement, direct invasion to adjacent organs,
bone involvement, regional and nonregional lymph node
metastases. Unclassified histology was a significant indicator
for poor prognosis. Median survival in patients with
advanced or metastatic unclassified renal cell carcinoma
was 4.3 months.29
Current Treatment Landscape for Non-clear Cell RCC
Nephrectomy plays an important and potentially curative
role in localized, and an important cytoreductive role
in metastatic, non-clear RCC given the suboptimal efficacy
of systemic therapy. In metastatic disease, cytoreductive
nephrectomy (CN) for non-clear cell RCC showed
significantly lower cancer-specific mortality and all-cause
mortality among 64% of the patients in the SEER database
between 2000 and 2009.1 Additionally, Vaishampayan
and colleagues analyzed advanced non-clear cell
RCC cases between 2000 and 2013 from SEER which
showed a higher risk of death in patients with non-clear
cell RCC when compared to clear cell with a median OS
5 and 7 months respectively.18 There were 10% more patients
with distant-stage non-clear cell RCC who under-
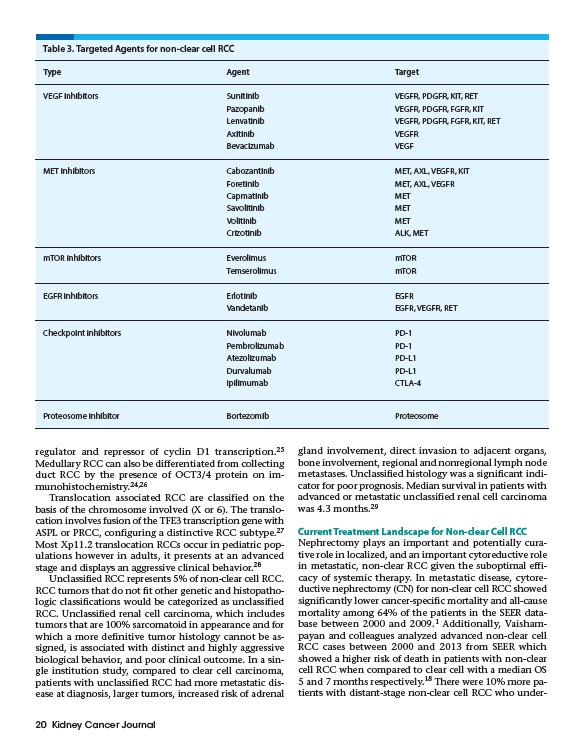
Table 3. Targeted Agents for non-clear cell RCC
Type Agent Target
VEGF inhibitors Sunitinib VEGFR, PDGFR, KIT, RET
Pazopanib VEGFR, PDGFR, FGFR, KIT
Lenvatinib VEGFR, PDGFR, FGFR, KIT, RET
Axitinib VEGFR
Bevacizumab VEGF
MET inhibitors Cabozantinib MET, AXL, VEGFR, KIT
Foretinib MET, AXL, VEGFR
Capmatinib MET
Savolitinib MET
Volitinib MET
Crizotinib ALK, MET
mTOR inhibitors Everolimus mTOR
Temserolimus mTOR
EGFR inhibitors Erlotinib EGFR
Vandetanib EGFR, VEGFR, RET
Checkpoint inhibitors Nivolumab PD-1
Pembrolizumab PD-1
Atezolizumab PD-L1
Durvalumab PD-L1
Ipilimumab CTLA-4
Proteosome inhibitor Bortezomib Proteosome