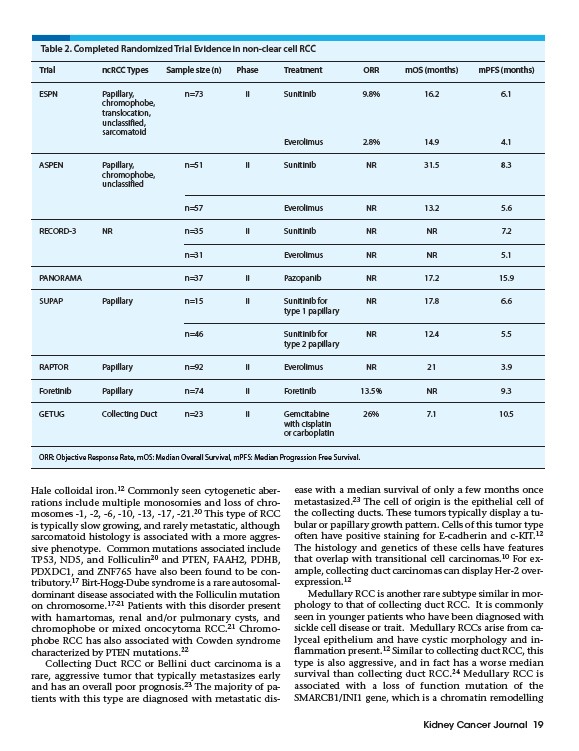
Table 2. Completed Randomized Trial Evidence in non-clear cell RCC
Trial ncRCC Types Sample size (n) Phase Treatment ORR mOS (months) mPFS (months)
ESPN Papillary, n=73 II Sunitinib 9.8% 16.2 6.1
Kidney Cancer Journal 19
Hale colloidal iron.12 Commonly seen cytogenetic aberrations
include multiple monosomies and loss of chromosomes
-1, -2, -6, -10, -13, -17, -21.20 This type of RCC
is typically slow growing, and rarely metastatic, although
sarcomatoid histology is associated with a more aggressive
phenotype. Common mutations associated include
TP53, ND5, and Folliculin20 and PTEN, FAAH2, PDHB,
PDXDC1, and ZNF765 have also been found to be contributory.
17 Birt-Hogg-Dube syndrome is a rare autosomaldominant
disease associated with the Folliculin mutation
on chromosome.17-21 Patients with this disorder present
with hamartomas, renal and/or pulmonary cysts, and
chromophobe or mixed oncocytoma RCC.21 Chromophobe
RCC has also associated with Cowden syndrome
characterized by PTEN mutations.22
Collecting Duct RCC or Bellini duct carcinoma is a
rare, aggressive tumor that typically metastasizes early
and has an overall poor prognosis.23 The majority of patients
with this type are diagnosed with metastatic disease
with a median survival of only a few months once
metastasized.23 The cell of origin is the epithelial cell of
the collecting ducts. These tumors typically display a tubular
or papillary growth pattern. Cells of this tumor type
often have positive staining for E-cadherin and c-KIT.12
The histology and genetics of these cells have features
that overlap with transitional cell carcinomas.10 For example,
collecting duct carcinomas can display Her-2 overexpression.
12
Medullary RCC is another rare subtype similar in morphology
to that of collecting duct RCC. It is commonly
seen in younger patients who have been diagnosed with
sickle cell disease or trait. Medullary RCCs arise from calyceal
epithelium and have cystic morphology and inflammation
present.12 Similar to collecting duct RCC, this
type is also aggressive, and in fact has a worse median
survival than collecting duct RCC.24 Medullary RCC is
associated with a loss of function mutation of the
SMARCB1/INI1 gene, which is a chromatin remodelling
chromophobe,
translocation,
unclassified,
sarcomatoid
Everolimus 2.8% 14.9 4.1
ASPEN Papillary, n=51 II Sunitinib NR 31.5 8.3
chromophobe,
unclassified
n=57 Everolimus NR 13.2 5.6
RECORD-3 NR n=35 II Sunitinib NR NR 7.2
n=31 Everolimus NR NR 5.1
PANORAMA n=37 II Pazopanib NR 17.2 15.9
SUPAP Papillary n=15 II Sunitinib for NR 17.8 6.6
type 1 papillary
n=46 Sunitinib for NR 12.4 5.5
type 2 papillary
RAPTOR Papillary n=92 II Everolimus NR 21 3.9
Foretinib Papillary n=74 II Foretinib 13.5% NR 9.3
GETUG Collecting Duct n=23 II Gemcitabine 26% 7.1 10.5
with cisplatin
or carboplatin
ORR: Objective Response Rate, mOS: Median Overall Survival, mPFS: Median Progression Free Survival.