AKT
TSC1
TSC2
proach has been delineated in numerous trials. These reports
share a common hypothesis: the most important
mechanism involved in the pathogenesis of sporadic and
VHL-related RCC is the overexpression of angiogenic
growth factors stimulated by HIF-1 alpha and HIF-2 alpha
after inactivation of VHL (Fig. 3). Thus, a growing literature
has drawn a connection between the treatment of
sporadic RCC and the VHL-related syndromes. For example,
in a landmark paper, Kaelin,13 suggested that mutations
or promoter hypermethylation of the VHL gene
may be frequently found in sporadic clear cell RCC. It is
a logical step then to suggest there may be a correlation
with sensitivity to antiangiogenic treatment.
14 Kidney Cancer Journal
Sunitinib
There are emerging data on the benefit of
TKIs in VHL disease patients with progressive
disease in the kidneys or other sites.
The clinical trials have primarily focused
on the use of two TKIs, sunitinib and pazopanib;
however, other agents have also
undergone study such as bevacizumab and
ranibizumab. In their retrospective analysis,
Roma et al14 evaluated progression-free
survival in 14 patients with geneticallyconfirmed
VHL treated for a histological diagnosis
of multifocal or advanced RCC.
After administering sunitinib as a first systemic
treatment, Roma et al recorded 9
partial responses (64.3%) and 5 stabilizations
of disease with a PFS of 71.4% at 2
years. All evaluable hemangioblastomas remained
stable. More encouraging were the
radiological responses observed not only in
renal lesions but also in pancreatic, adrenal,
hepatic, pulmonary and subcutaneous
nodules as well as in some cystic lesions,
which represents a wide spectrum of VHLrelated
lesions.
In a prospective trial,15 we evaluated the
safety and efficacy of sunitinib in VHL patients
(NCT00330564) and examined the
expression of various receptors in archived
tissue. Of 18 RCCs, 33% responded favorably
although none of the hemangioblastomas
did. One intriguing finding concerned
the results of biomarker expression:
mean levels of VEGF receptors were lower
in hemangioblastoma than in RCC and
mean fibroblast growth factor receptor
(FGFR) activation state was higher in hemangioblastomas.
Why do organ-specific
VHL-derived lesions respond differently to
therapy? And what of the findings on fibroblast
growth factor (FGF) axis? To what
effect does do these differences affect organ
specific response rates? At this point in
time, we do not have clear answers to these
questions, but as previously stated, RCCs are true cancers,
whereas hemangioblastomas have no metastatic potential.
It could be that the differences are due to cancer-specific
genetic lesions or tissue-specific endothelial
differences. The results on FGF raise the possibility that
further studies should examine whether hemangioblastomas
could depend on FGF signaling and whether we
can identify biomarkers that will help us determine
whether agents will yield some benefit.
Dovitinib
To that end, we launched a phase II study14 (NCT01-
266070) in VHL patients to test the hypothesis that hemangioblastomas
would respond to dovitinib, which
MET
HIF-2a
PHD
HIF-1a
AMPK
PTEN
FLCN
mTORC1
mTORC2
PI3K
Rheb
pVHL
SDH
FH
Proteasome
E3 Ligase
Cell
nucleus
PcG
BAP1
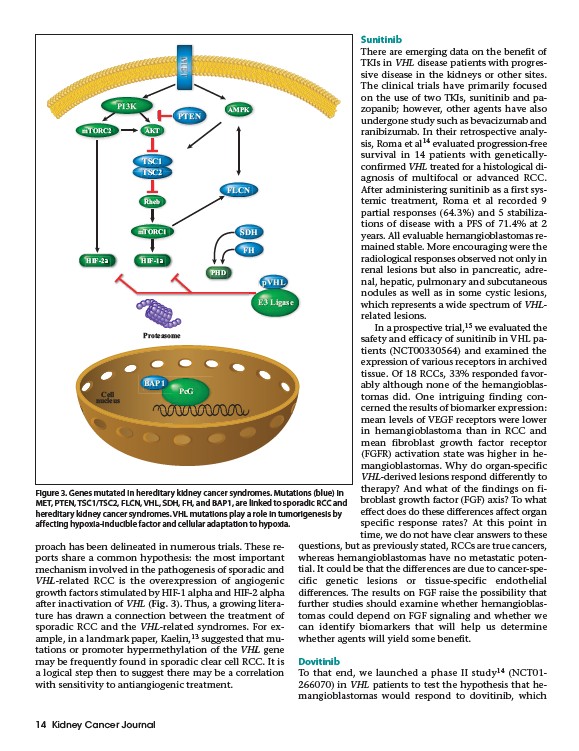
Figure 3. Genes mutated in hereditary kidney cancer syndromes. Mutations (blue) in
MET, PTEN, TSC1/TSC2, FLCN, VHL, SDH, FH, and BAP1, are linked to sporadic RCC and
hereditary kidney cancer syndromes. VHL mutations play a role in tumorigenesis by
affecting hypoxia-inducible factor and cellular adaptation to hypoxia.