Table 4. Table showing median OS in Favorable,
Intermediate, Poor and overall population.
Median OS
(n=665) (months)
IMDC Favorable 47.3
Intermediate 20.8
Poor 7.4
Overall 15.8
Kidney Cancer Journal 111
report. The proportion of patients with non-clear cell pathology,
which is usually associated with poorer outcome,
was also comparatively higher in this study cohort. In a
review done by Kidney Cancer UK in 2016 8, survival outcomes
in the UK as a whole is poorer compared to other
western advanced countries or European counterparts.
The possible contributing factors highlighted was the low
proportion of patients receiving more than one line of
treatment and the generally restricted overall number of
approved and effective treatment available during the
study period. Another relevant factor to the poor survival
outcome in this region is likely the very high proportion
(41%) of highly deprived neighborhoods served by this
referral center compared to only 6-7% in other parts of
England (ONS 2015)9 . The findings here indirectly highlighted
the absolute importance of public awareness and
early diagnosis to further improve survival outcome of
kidney cancer. The approval of several newer agents by
NICE in recent times including cabozantinib and ipilimumab
and nivolumab combination immunotherapy
among patients with I/P prognostic risk, for example, is
extremely timely and will likely bring about improvement
in survival outcome in general and for this region.
The outcome of mRCC patients with favorable prognostic
risk (IMDC or MSKCC) in this series is excellent
Table 3. Table showing median PFS in Favorable,
Intermediate, Poor risk and overall population.
Median PFS
(n=665) (months)
IMDC Favorable 29.2
Intermediate 13.0
Poor 4.1
Overall 10.5
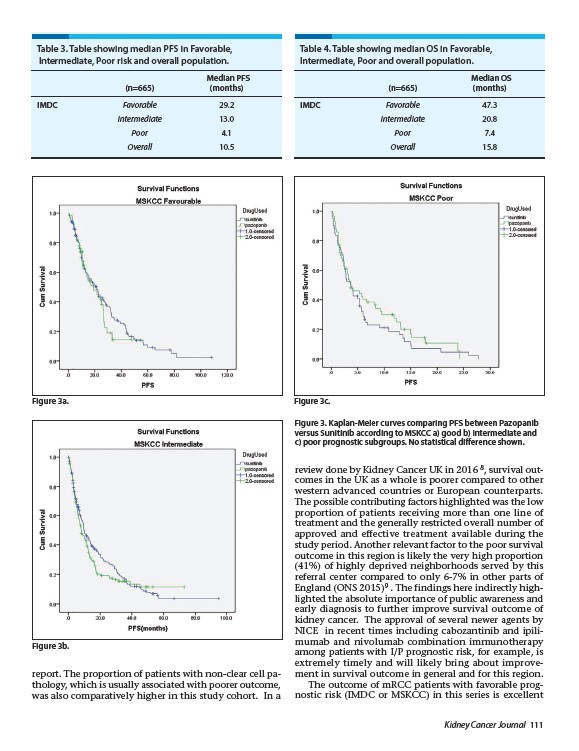
Figure 3a. Figure 3c.
Figure 3b.
Figure 3. Kaplan-Meier curves comparing PFS between Pazopanib
versus Sunitinib according to MSKCC a) good b) intermediate and
c) poor prognostic subgroups. No statistical difference shown.