Sunitinib Everolimus
Nivolumab + Ipilimumab
1992 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018
Kidney Cancer Journal 77
immunity, ultimately providing a stronger rationale for
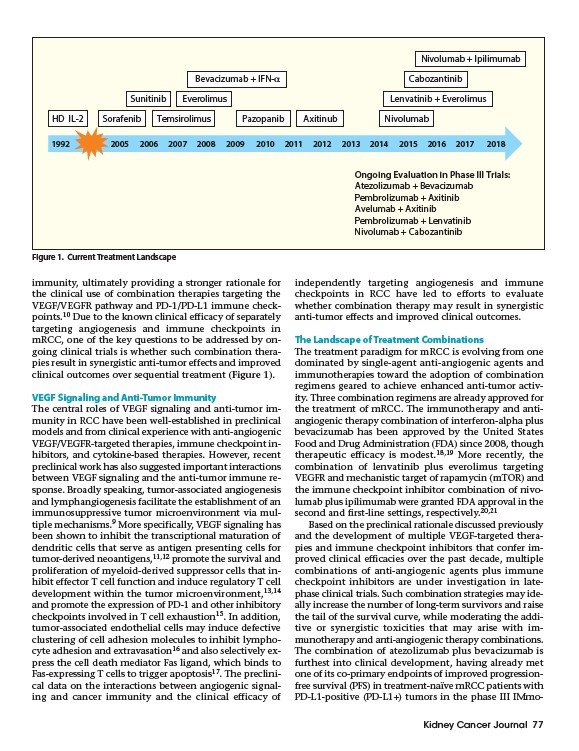
the clinical use of combination therapies targeting the
VEGF/VEGFR pathway and PD-1/PD-L1 immune checkpoints.
10 Due to the known clinical efficacy of separately
targeting angiogenesis and immune checkpoints in
mRCC, one of the key questions to be addressed by ongoing
clinical trials is whether such combination therapies
result in synergistic anti-tumor effects and improved
clinical outcomes over sequential treatment (Figure 1).
VEGF Signaling and Anti-Tumor Immunity
The central roles of VEGF signaling and anti-tumor immunity
in RCC have been well-established in preclinical
models and from clinical experience with anti-angiogenic
VEGF/VEGFR-targeted therapies, immune checkpoint inhibitors,
and cytokine-based therapies. However, recent
preclinical work has also suggested important interactions
between VEGF signaling and the anti-tumor immune response.
Broadly speaking, tumor-associated angiogenesis
and lymphangiogenesis facilitate the establishment of an
immunosuppressive tumor microenvironment via multiple
mechanisms.9 More specifically, VEGF signaling has
been shown to inhibit the transcriptional maturation of
dendritic cells that serve as antigen presenting cells for
tumor-derived neoantigens,11,12 promote the survival and
proliferation of myeloid-derived suppressor cells that inhibit
effector T cell function and induce regulatory T cell
development within the tumor microenvironment,13,14
and promote the expression of PD-1 and other inhibitory
checkpoints involved in T cell exhaustion15. In addition,
tumor-associated endothelial cells may induce defective
clustering of cell adhesion molecules to inhibit lymphocyte
adhesion and extravasation16 and also selectively express
the cell death mediator Fas ligand, which binds to
Fas-expressing T cells to trigger apoptosis17. The preclinical
data on the interactions between angiogenic signaling
and cancer immunity and the clinical efficacy of
independently targeting angiogenesis and immune
checkpoints in RCC have led to efforts to evaluate
whether combination therapy may result in synergistic
anti-tumor effects and improved clinical outcomes.
The Landscape of Treatment Combinations
The treatment paradigm for mRCC is evolving from one
dominated by single-agent anti-angiogenic agents and
immunotherapies toward the adoption of combination
regimens geared to achieve enhanced anti-tumor activity.
Three combination regimens are already approved for
the treatment of mRCC. The immunotherapy and antiangiogenic
therapy combination of interferon-alpha plus
bevacizumab has been approved by the United States
Food and Drug Administration (FDA) since 2008, though
therapeutic efficacy is modest.18,19 More recently, the
combination of lenvatinib plus everolimus targeting
VEGFR and mechanistic target of rapamycin (mTOR) and
the immune checkpoint inhibitor combination of nivolumab
plus ipilimumab were granted FDA approval in the
second and first-line settings, respectively.20,21
Based on the preclinical rationale discussed previously
and the development of multiple VEGF-targeted therapies
and immune checkpoint inhibitors that confer improved
clinical efficacies over the past decade, multiple
combinations of anti-angiogenic agents plus immune
checkpoint inhibitors are under investigation in latephase
clinical trials. Such combination strategies may ideally
increase the number of long-term survivors and raise
the tail of the survival curve, while moderating the additive
or synergistic toxicities that may arise with immunotherapy
and anti-angiogenic therapy combinations.
The combination of atezolizumab plus bevacizumab is
furthest into clinical development, having already met
one of its co-primary endpoints of improved progressionfree
survival (PFS) in treatment-naïve mRCC patients with
PD-L1-positive (PD-L1+) tumors in the phase III IMmo-
HD IL-2 Sorafenib
Bevacizumab + IFN-α Cabozantinib
Lenvatinib + Everolimus
Temsirolimus Pazopanib Axitinub Nivolumab
Ongoing Evaluation in Phase III Trials:
Atezolizumab + Bevacizumab
Pembrolizumab + Axitinib
Avelumab + Axitinib
Pembrolizumab + Lenvatinib
Nivolumab + Cabozantinib
Figure 1. Current Treatment Landscape