Published
Sunitinib
Untreated RCC NCT03141177
NCT02320821
Sunitinib
greater than the ULN. Patients were segregated into three
risk categories: the favorable-risk group (no prognostic factors;
n = 133), in which median OS (mOS) was not reached
and 2-year OS (2y OS) was 75%; the intermediate-risk
group (one or two prognostic factors; n = 301), in which
mOS was 27 months and 2y OS was 53%; and the poorrisk
group (three to six prognostic factors; n = 152), in
which mOS was 8.8 months and 2y OS was 7%. All these
prognostic factors may reflect increased tumor burden,
aggressive tumor biology, and/or paraneoplastic processes,
which might account for their high discriminatory
power.4–6 This classi- fication is widely applicable, as it involved
real-world patients from multiple sites, and was
validated in additional cohorts and prospective clinical
trials.7,8
Sunitinib vs Pazopanib vs Cabozantinib:
TKI Monotherapy Comparisons, Criteria for Selection
TKI monotherapy has been the mainstay of therapy for
over 10 years. Evidence is still accumulating from prospective
trials on the relative merits of these three TKIs,
while emerging data highlight their distinct activity and
safety profiles. Until 2017, sunitinib and pazopanib were
84 Kidney Cancer Journal
Untreated RCC
NCT02853331
Untreated RCC
Lenvatinib +
Pembrolizumab
Lenvatinib +
Everolimus
the two approved agents used most often in the first-line
setting. The COMPARZ phase 3 non-inferiority study
showed that pazopanib was not inferior to sunitinib in
term of PFS (primary endpoint) and OS (secondary endpoint).
9 Objective responses were higher in the pazopanib
group. Although the study found similar rates of dose reduction
and drug discontinuation due to adverse events,
differences were revealed in safety profiles: patients assigned
to pazopanib had less fatigue, gastrointestinal adverse
events, hand-foot syndrome, mouth sores, but
experienced higher rates of liver toxicity. Eleven out of 14
quality of life metrics favored pazopanib over sunitinib.
Therefore, the safety profile would be key to determine
therapeutic strategies in the setting of similar efficacy.10,11
Further evidence regarding the importance of patientreported
outcomes and how they can help treatment
choices came from the phase II cross-over trial PISCES.12
This study raised the importance of patient evaluation to
assess differences in tolerability that may not be accurately
captured by the standard measures used for adverse
event reporting. This could be especially true in the case
of low-grade but chronic toxicities, that can still impact
the quality of life of patients.13 Pazopanib was preferred
Untreated RCC
NCT02682006
Atezolizumab +
Bevacizumab
Axitinib +
Avelumab
Sunitinib
Axitinib +
Pembrolizumab
Sunitinib
Cabozantinib +
Nivolumab
Sunitinib
Presented
Completed
Accrual
Completed
Accrual
Accruing
Untreated RCC
NCT02811861
Accruing
Nivolumab
Sunitinib
Untreated RCC
NCT02231749
Nivolumab +
Ipilimumab x 4
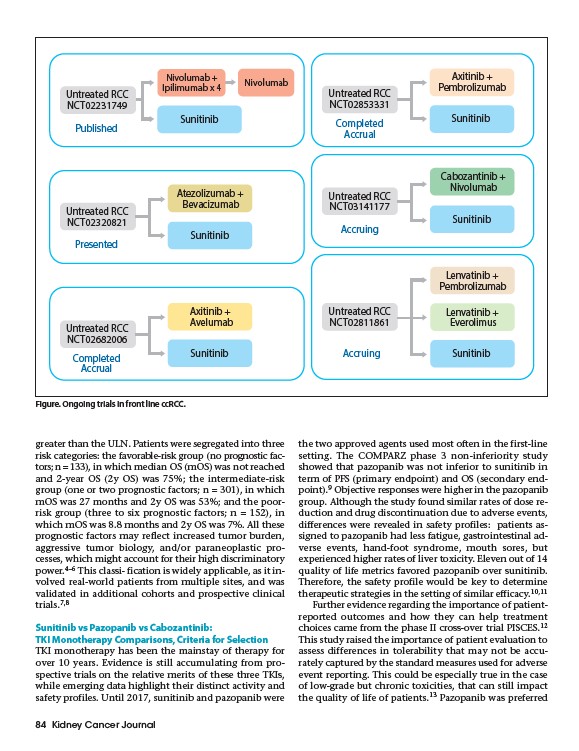
Figure. Ongoing trials in front line ccRCC.