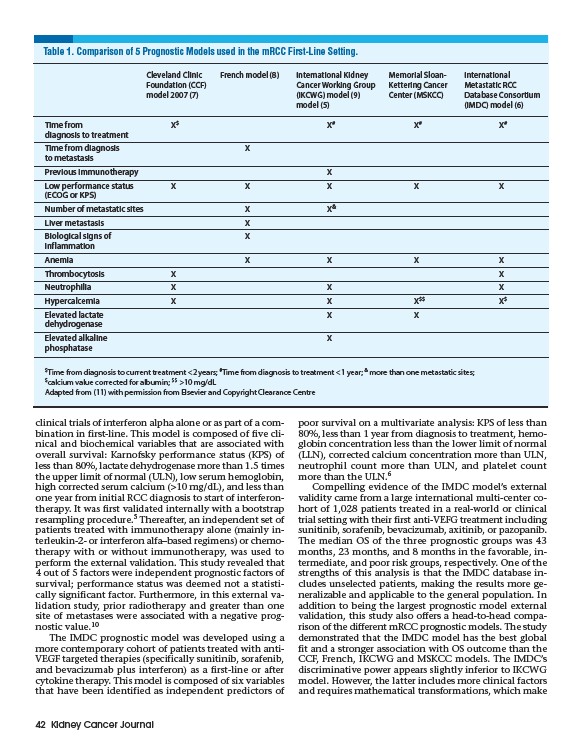
Table 1. Comparison of 5 Prognostic Models used in the mRCC First-Line Setting.
Cleveland Clinic French model (8) International Kidney Memorial Sloan- International
Foundation (CCF) Cancer Working Group Kettering Cancer Metastatic RCC
model 2007 (7) (IKCWG) model (9) Center (MSKCC) Database Consortium
Time from X$ X# X# X#
diagnosis to treatment
Time from diagnosis X
to metastasis
Previous immunotherapy X
Low performance status X X X X X
(ECOG or KPS)
Number of metastatic sites X X&
Liver metastasis X
Biological signs of X
inflammation
Anemia X X X X
Thrombocytosis X X
Neutrophilia X X X
Hypercalcemia X X X$$ X$
Elevated lactate X X
dehydrogenase
Elevated alkaline X
phosphatase
clinical trials of interferon alpha alone or as part of a combination
in first-line. This model is composed of five clinical
and biochemical variables that are associated with
overall survival: Karnofsky performance status (KPS) of
less than 80%, lactate dehydrogenase more than 1.5 times
the upper limit of normal (ULN), low serum hemoglobin,
high corrected serum calcium (>10 mg/dL), and less than
one year from initial RCC diagnosis to start of interferontherapy.
It was first validated internally with a bootstrap
resampling procedure.5 Thereafter, an independent set of
patients treated with immunotherapy alone (mainly interleukin
2- or interferon alfa–based regimens) or chemotherapy
with or without immunotherapy, was used to
perform the external validation. This study revealed that
4 out of 5 factors were independent prognostic factors of
survival; performance status was deemed not a statistically
significant factor. Furthermore, in this external validation
study, prior radiotherapy and greater than one
site of metastases were associated with a negative prognostic
value.10
The IMDC prognostic model was developed using a
more contemporary cohort of patients treated with anti-
VEGF targeted therapies (specifically sunitinib, sorafenib,
and bevacizumab plus interferon) as a first-line or after
cytokine therapy. This model is composed of six variables
that have been identified as independent predictors of
42 Kidney Cancer Journal
model (5) (IMDC) model (6)
poor survival on a multivariate analysis: KPS of less than
80%, less than 1 year from diagnosis to treatment, hemoglobin
concentration less than the lower limit of normal
(LLN), corrected calcium concentration more than ULN,
neutrophil count more than ULN, and platelet count
more than the ULN.6
Compelling evidence of the IMDC model’s external
validity came from a large international multi-center cohort
of 1,028 patients treated in a real-world or clinical
trial setting with their first anti-VEFG treatment including
sunitinib, sorafenib, bevacizumab, axitinib, or pazopanib.
The median OS of the three prognostic groups was 43
months, 23 months, and 8 months in the favorable, intermediate,
and poor risk groups, respectively. One of the
strengths of this analysis is that the IMDC database includes
unselected patients, making the results more generalizable
and applicable to the general population. In
addition to being the largest prognostic model external
validation, this study also offers a head-to-head comparison
of the different mRCC prognostic models. The study
demonstrated that the IMDC model has the best global
fit and a stronger association with OS outcome than the
CCF, French, IKCWG and MSKCC models. The IMDC’s
discriminative power appears slightly inferior to IKCWG
model. However, the latter includes more clinical factors
and requires mathematical transformations, which make
$Time from diagnosis to current treatment <2 years; #Time from diagnosis to treatment <1 year; & more than one metastatic sites;
$calcium value corrected for albumin; $$ >10 mg/dL
Adapted from (11) with permission from Elsevier and Copyright Clearance Centre