Kidney Cancer Journal 43
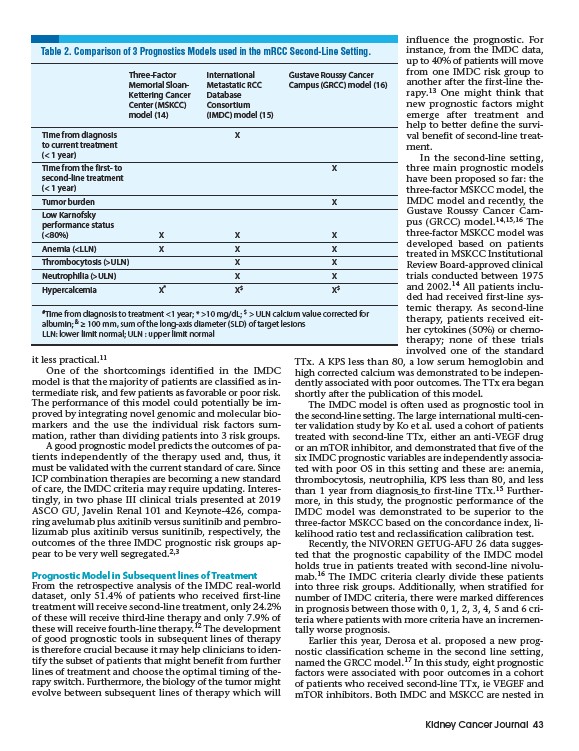
Table 2. Comparison of 3 Prognostics Models used in the mRCC Second-Line Setting.
Time from diagnosis X
to current treatment
(< 1 year)
Time from the first- to X
second-line treatment
(< 1 year)
Tumor burden X
Low Karnofsky
performance status
(<80%) X X X
Anemia (<LLN) X X X
Thrombocytosis (>ULN) X X
Neutrophilia (>ULN) X X
Hypercalcemia X* X$ X$
it less practical.11
Three-Factor International Gustave Roussy Cancer
Memorial Sloan- Metastatic RCC Campus (GRCC) model (16)
Kettering Cancer Database
Center (MSKCC) Consortium
model (14) (IMDC) model (15)
One of the shortcomings identified in the IMDC
model is that the majority of patients are classified as intermediate
risk, and few patients as favorable or poor risk.
The performance of this model could potentially be improved
by integrating novel genomic and molecular biomarkers
and the use the individual risk factors sum-
mation, rather than dividing patients into 3 risk groups.
A good prognostic model predicts the outcomes of patients
independently of the therapy used and, thus, it
must be validated with the current standard of care. Since
ICP combination therapies are becoming a new standard
of care, the IMDC criteria may require updating. Interestingly,
in two phase III clinical trials presented at 2019
ASCO GU, Javelin Renal 101 and Keynote-426, comparing
avelumab plus axitinib versus sunitinib and pembrolizumab
plus axitinib versus sunitinib, respectively, the
outcomes of the three IMDC prognostic risk groups appear
to be very well segregated.2,3
Prognostic Model in Subsequent lines of Treatment
From the retrospective analysis of the IMDC real-world
dataset, only 51.4% of patients who received first-line
treatment will receive second-line treatment, only 24.2%
of these will receive third-line therapy and only 7.9% of
these will receive fourth-line therapy.12 The development
of good prognostic tools in subsequent lines of therapy
is therefore crucial because it may help clinicians to identify
the subset of patients that might benefit from further
lines of treatment and choose the optimal timing of therapy
switch. Furthermore, the biology of the tumor might
evolve between subsequent lines of therapy which will
influence the prognostic. For
instance, from the IMDC data,
up to 40% of patients will move
from one IMDC risk group to
another after the first-line therapy.
13 One might think that
new prognostic factors might
emerge after treatment and
help to better define the survival
benefit of second-line treatment.
In the second-line setting,
three main prognostic models
have been proposed so far: the
three-factor MSKCC model, the
IMDC model and recently, the
Gustave Roussy Cancer Campus
(GRCC) model.14,15,16 The
three-factor MSKCC model was
developed based on patients
treated in MSKCC Institutional
Review Board-approved clinical
trials conducted between 1975
and 2002.14 All patients included
had received first-line systemic
therapy. As second-line
therapy, patients received either
cytokines (50%) or chemotherapy;
none of these trials
involved one of the standard
TTx. A KPS less than 80, a low serum hemoglobin and
high corrected calcium was demonstrated to be independently
associated with poor outcomes. The TTx era began
shortly after the publication of this model.
The IMDC model is often used as prognostic tool in
the second-line setting. The large international multi-center
validation study by Ko et al. used a cohort of patients
treated with second-line TTx, either an anti-VEGF drug
or an mTOR inhibitor, and demonstrated that five of the
six IMDC prognostic variables are independently associated
with poor OS in this setting and these are: anemia,
thrombocytosis, neutrophilia, KPS less than 80, and less
than 1 year from diagnosis to first-line TTx.15 Furthermore,
in this study, the prognostic performance of the
IMDC model was demonstrated to be superior to the
three-factor MSKCC based on the concordance index, likelihood
ratio test and reclassification calibration test.
Recently, the NIVOREN GETUG-AFU 26 data suggested
that the prognostic capability of the IMDC model
holds true in patients treated with second-line nivolumab.
16 The IMDC criteria clearly divide these patients
into three risk groups. Additionally, when stratified for
number of IMDC criteria, there were marked differences
in prognosis between those with 0, 1, 2, 3, 4, 5 and 6 criteria
where patients with more criteria have an incrementally
worse prognosis.
Earlier this year, Derosa et al. proposed a new prognostic
classification scheme in the second line setting,
named the GRCC model.17 In this study, eight prognostic
factors were associated with poor outcomes in a cohort
of patients who received second-line TTx, ie VEGEF and
mTOR inhibitors. Both IMDC and MSKCC are nested in
#
Time from diagnosis to treatment <1 year; * >10 mg/dL; $ > ULN calcium value corrected for
albumin; & ≥ 100 mm, sum of the long-axis diameter (SLD) of target lesions
LLN: lower limit normal; ULN : upper limit normal