1
16 NAUI Nitrox Diver
Our body does not use the nitrogen we breathe–we
inhale it and exhale it. Being inert, nitrogen is unaltered
in the respiratory process and, for all practical purposes,
quantitatively obeys purely physical laws. Because it is
soluble in water and fats, some nitrogen passes through
our lungs into our circulatory system and is then
absorbed in the tissues of our body. A certain amount
of nitrogen naturally pervades our tissues at all times.
Right now, your body is saturated with dissolved nitrogen
for the surrounding air pressure. When diving, the
increased pressure of depth causes additional nitrogen
to be dissolved in our tissues. If the nitrogen loading is
excessive, it can cause nitrogen narcosis during the dive
or, if the ascent is too rapid, decompression sickness after
you surface (or in extreme cases, as you approach the
surface).
Drawbacks of nitrogen were recognized long before
the development of scuba. In 1878, French physiologist
Paul Bert established that nitrogen, liberated as bubbles
following sudden decompression, was the cause of
decompression sickness. Nitrogen bubbles collect and
expand, and the tissue or neurological insult that results
presents as signs and symptoms of the bends.
In the early twentieth century, John Scott Haldane
developed a quantitative model for nitrogen loading, and
devised tables that set safe time limits for single dives and
stage decompression schedules for dives that exceeded
the limits.
As noted above, one solution to the nitrogen
problem seems obvious–breathe less nitrogen. If the air
we normally breathe is one-fifth oxygen and four-fifths
nitrogen, why not just take out some of the nitrogen and
go diving. This is not a new idea either. Our knowledge
of the physiological effects of the gases we breathe
has grown over a long period of time, and we are still
learning.
Pure oxygen has limited applicability in diving.
In the 1870s, the same Paul Bert, in a separate set of
experiments, established that breathing pure oxygen
under pressure could cause convulsions and death.
However, the hazards were not widely known for some
time, and early scuba units were most often oxygen
rebreathers that re-circulated pure oxygen while
removing carbon dioxide. Seemingly, the seriousness of
the hyperbaric oxygen problems in diving was not fully
appreciated until a number of oxygen-toxicity accidents
among military divers early in World War II.
As early as 1919, it was suggested that nitrogen could
be replaced by helium to increase divers’ operational
working depth. Work on helium-oxygen mixtures
began in earnest in the 1930s. In 1937, Max Gene Nohl,
breathing a helium-oxygen mixture and using a suit of
his own design, dove to a depth of 128 meters (420 feet)
in Lake Michigan. The first practical test of heliox was
the U.S. Navy’s salvage of the submarine USS Squalus
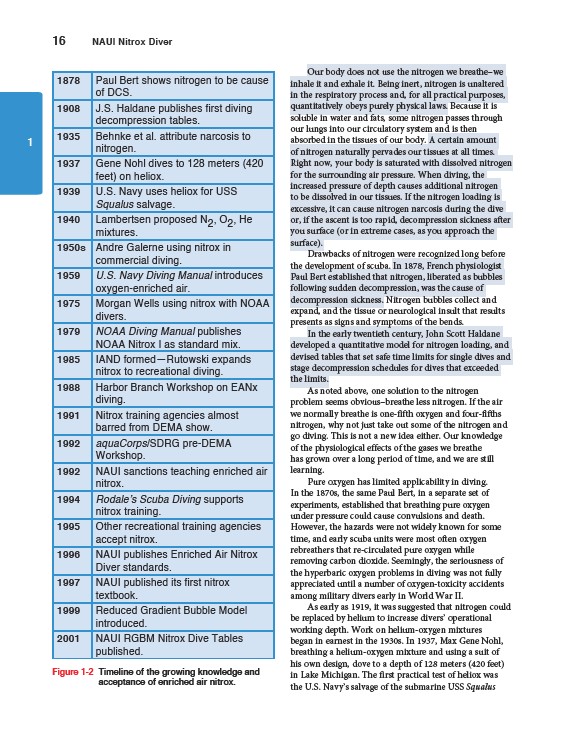
1878 Paul Bert shows nitrogen to be cause
of DCS.
1908 J.S. Haldane publishes first diving
decompression tables.
1935 Behnke et al. attribute narcosis to
nitrogen.
1937 Gene Nohl dives to 128 meters (420
feet) on heliox.
1939 U.S. Navy uses heliox for USS
Squalus salvage.
1940 Lambertsen proposed N2, O2, He
mixtures.
1950s Andre Galerne using nitrox in
commercial diving.
1959 U.S. Navy Diving Manual introduces
oxygen-enriched air.
1975 Morgan Wells using nitrox with NOAA
divers.
1979 NOAA Diving Manual publishes
NOAA Nitrox I as standard mix.
1985 IAND formed—Rutowski expands
nitrox to recreational diving.
1988 Harbor Branch Workshop on EANx
diving.
1991 Nitrox training agencies almost
barred from DEMA show.
1992 aquaCorps/SDRG pre-DEMA
Workshop.
1992 NAUI sanctions teaching enriched air
nitrox.
1994 Rodale’s Scuba Diving supports
nitrox training.
1995 Other recreational training agencies
accept nitrox.
1996 NAUI publishes Enriched Air Nitrox
Diver standards.
1997 NAUI published its first nitrox
textbook.
1999 Reduced Gradient Bubble Model
introduced.
2001 NAUI RGBM Nitrox Dive Tables
published.
Figure 1-2 Timeline of the growing knowledge and
acceptance of enriched air nitrox.