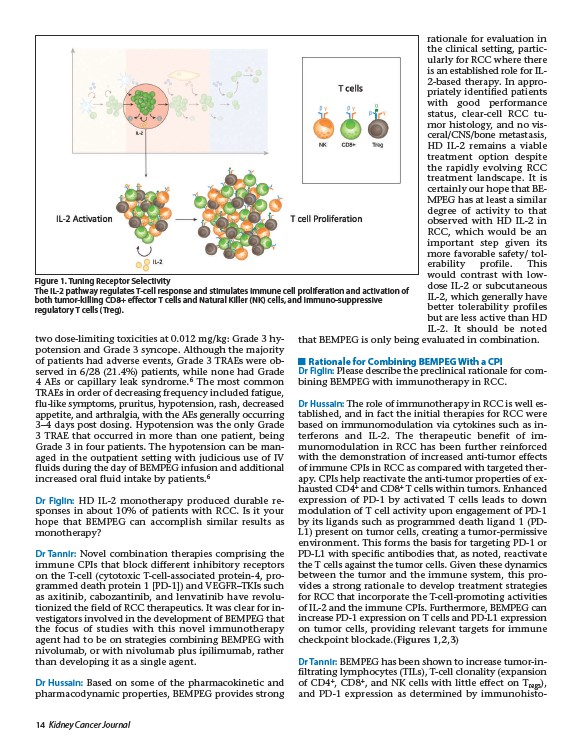
Figure 1. Tuning Receptor Selectivity
The IL-2 pathway regulates T-cell response and stimulates immune cell proliferation and activation of
both tumor-killing CD8+ effector T cells and Natural Killer (NK) cells, and immuno-suppressive
regulatory T cells (Treg).
two dose-limiting toxicities at 0.012 mg/kg: Grade 3 hypotension
and Grade 3 syncope. Although the majority
of patients had adverse events, Grade 3 TRAEs were observed
in 6/28 (21.4%) patients, while none had Grade
4 AEs or capillary leak syndrome.6 The most common
TRAEs in order of decreasing frequency included fatigue,
flu-like symptoms, pruritus, hypotension, rash, decreased
appetite, and arthralgia, with the AEs generally occurring
3–4 days post dosing. Hypotension was the only Grade
3 TRAE that occurred in more than one patient, being
Grade 3 in four patients. The hypotension can be managed
in the outpatient setting with judicious use of IV
fluids during the day of BEMPEG infusion and additional
increased oral fluid intake by patients.6
Dr Figlin: HD IL-2 monotherapy produced durable responses
in about 10% of patients with RCC. Is it your
hope that BEMPEG can accomplish similar results as
monotherapy?
Dr Tannir: Novel combination therapies comprising the
immune CPIs that block different inhibitory receptors
on the T-cell (cytotoxic T-cell-associated protein-4, programmed
death protein 1 PD-1) and VEGFR–TKIs such
as axitinib, cabozantinib, and lenvatinib have revolutionized
the field of RCC therapeutics. It was clear for investigators
involved in the development of BEMPEG that
the focus of studies with this novel immunotherapy
agent had to be on strategies combining BEMPEG with
nivolumab, or with nivolumab plus ipilimumab, rather
than developing it as a single agent.
Dr Hussain: Based on some of the pharmacokinetic and
pharmacodynamic properties, BEMPEG provides strong
14 Kidney Cancer Journal
rationale for evaluation in
the clinical setting, particularly
for RCC where there
is an established role for IL-
2-based therapy. In appropriately
identified patients
with good performance
status, clear-cell RCC tumor
histology, and no visceral/
CNS/bone metastasis,
HD IL-2 remains a viable
treatment option despite
the rapidly evolving RCC
treatment landscape. It is
certainly our hope that BEMPEG
has at least a similar
degree of activity to that
observed with HD IL-2 in
RCC, which would be an
important step given its
more favorable safety/ tolerability
profile. This
would contrast with lowdose
IL-2 or subcutaneous
IL-2, which generally have
better tolerability profiles
but are less active than HD
IL-2. It should be noted
that BEMPEG is only being evaluated in combination.
Rationale for Combining BEMPEG With a CPI
Dr Figlin: Please describe the preclinical rationale for combining
BEMPEG with immunotherapy in RCC.
Dr Hussain: The role of immunotherapy in RCC is well established,
and in fact the initial therapies for RCC were
based on immunomodulation via cytokines such as interferons
and IL-2. The therapeutic benefit of immunomodulation
in RCC has been further reinforced
with the demonstration of increased anti-tumor effects
of immune CPIs in RCC as compared with targeted therapy.
CPIs help reactivate the anti-tumor properties of exhausted
CD4+ and CD8+ T cells within tumors. Enhanced
expression of PD-1 by activated T cells leads to down
modulation of T cell activity upon engagement of PD-1
by its ligands such as programmed death ligand 1 (PDL1)
present on tumor cells, creating a tumor-permissive
environment. This forms the basis for targeting PD-1 or
PD-L1 with specific antibodies that, as noted, reactivate
the T cells against the tumor cells. Given these dynamics
between the tumor and the immune system, this provides
a strong rationale to develop treatment strategies
for RCC that incorporate the T-cell-promoting activities
of IL-2 and the immune CPIs. Furthermore, BEMPEG can
increase PD-1 expression on T cells and PD-L1 expression
on tumor cells, providing relevant targets for immune
checkpoint blockade.(Figures 1,2,3)
Dr Tannir: BEMPEG has been shown to increase tumor-infiltrating
lymphocytes (TILs), T-cell clonality (expansion
of CD4+, CD8+, and NK cells with little effect on Tregs),
and PD-1 expression as determined by immunohisto-