Kidney Cancer Journal 15
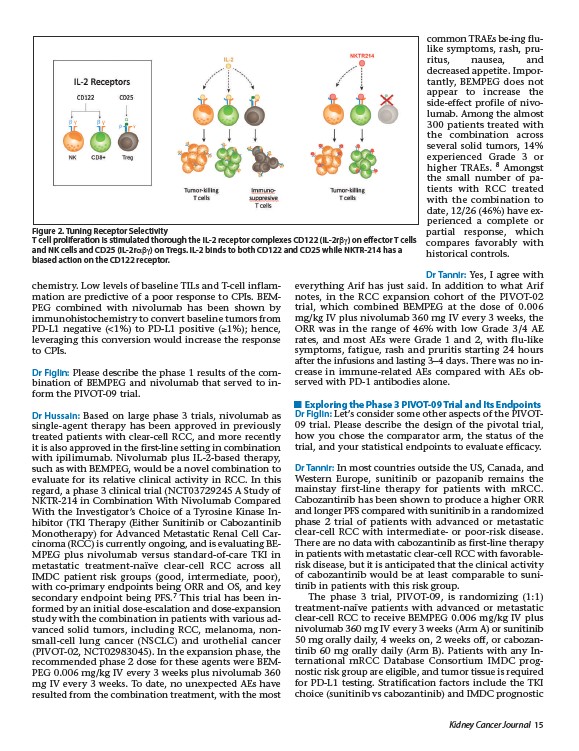
Figure 2. Tuning Receptor Selectivity
T cell proliferation is stimulated thorough the IL-2 receptor complexes CD122 (IL-2rbg) on effector T cells
and NK cells and CD25 (IL-2r��bg) on Tregs. IL-2 binds to both CD122 and CD25 while NKTR-214 has a
biased action on the CD122 receptor.
chemistry. Low levels of baseline TILs and T-cell inflammation
are predictive of a poor response to CPIs. BEMPEG
combined with nivolumab has been shown by
immunohistochemistry to convert baseline tumors from
PD-L1 negative (<1%) to PD-L1 positive (��1%); hence,
leveraging this conversion would increase the response
to CPIs.
Dr Figlin: Please describe the phase 1 results of the combination
of BEMPEG and nivolumab that served to inform
the PIVOT-09 trial.
Dr Hussain: Based on large phase 3 trials, nivolumab as
single-agent therapy has been approved in previously
treated patients with clear-cell RCC, and more recently
it is also approved in the first-line setting in combination
with ipilimumab. Nivolumab plus IL-2-based therapy,
such as with BEMPEG, would be a novel combination to
evaluate for its relative clinical activity in RCC. In this
regard, a phase 3 clinical trial (NCT03729245 A Study of
NKTR-214 in Combination With Nivolumab Compared
With the Investigator’s Choice of a Tyrosine Kinase Inhibitor
(TKI Therapy (Either Sunitinib or Cabozantinib
Monotherapy) for Advanced Metastatic Renal Cell Carcinoma
(RCC) is currently ongoing, and is evaluating BEMPEG
plus nivolumab versus standard-of-care TKI in
metastatic treatment-naïve clear-cell RCC across all
IMDC patient risk groups (good, intermediate, poor),
with co-primary endpoints being ORR and OS, and key
secondary endpoint being PFS.7 This trial has been informed
by an initial dose-escalation and dose-expansion
study with the combination in patients with various advanced
solid tumors, including RCC, melanoma, nonsmall
cell lung cancer (NSCLC) and urothelial cancer
(PIVOT-02, NCT02983045). In the expansion phase, the
recommended phase 2 dose for these agents were BEMPEG
0.006 mg/kg IV every 3 weeks plus nivolumab 360
mg IV every 3 weeks. To date, no unexpected AEs have
resulted from the combination treatment, with the most
common TRAEs be-ing flulike
symptoms, rash, pruritus,
nausea, and
decreased appetite. Importantly,
BEMPEG does not
appear to increase the
side-effect profile of nivolumab.
Among the almost
300 patients treated with
the combination across
several solid tumors, 14%
experienced Grade 3 or
higher TRAEs. 8 Amongst
the small number of patients
with RCC treated
with the combination to
date, 12/26 (46%) have experienced
a complete or
partial response, which
compares favorably with
historical controls.
Dr Tannir: Yes, I agree with
everything Arif has just said. In addition to what Arif
notes, in the RCC expansion cohort of the PIVOT-02
trial, which combined BEMPEG at the dose of 0.006
mg/kg IV plus nivolumab 360 mg IV every 3 weeks, the
ORR was in the range of 46% with low Grade 3/4 AE
rates, and most AEs were Grade 1 and 2, with flu-like
symptoms, fatigue, rash and pruritis starting 24 hours
after the infusions and lasting 3–4 days. There was no increase
in immune-related AEs compared with AEs observed
with PD-1 antibodies alone.
Exploring the Phase 3 PIVOT-09 Trial and Its Endpoints
Dr Figlin: Let’s consider some other aspects of the PIVOT-
09 trial. Please describe the design of the pivotal trial,
how you chose the comparator arm, the status of the
trial, and your statistical endpoints to evaluate efficacy.
Dr Tannir: In most countries outside the US, Canada, and
Western Europe, sunitinib or pazopanib remains the
mainstay first-line therapy for patients with mRCC.
Cabozantinib has been shown to produce a higher ORR
and longer PFS compared with sunitinib in a randomized
phase 2 trial of patients with advanced or metastatic
clear-cell RCC with intermediate- or poor-risk disease.
There are no data with cabozantinib as first-line therapy
in patients with metastatic clear-cell RCC with favorablerisk
disease, but it is anticipated that the clinical activity
of cabozantinib would be at least comparable to sunitinib
in patients with this risk group.
The phase 3 trial, PIVOT-09, is randomizing (1:1)
treatment-naïve patients with advanced or metastatic
clear-cell RCC to receive BEMPEG 0.006 mg/kg IV plus
nivolumab 360 mg IV every 3 weeks (Arm A) or sunitinib
50 mg orally daily, 4 weeks on, 2 weeks off, or cabozantinib
60 mg orally daily (Arm B). Patients with any International
mRCC Database Consortium IMDC prog-
nostic risk group are eligible, and tumor tissue is required
for PD-L1 testing. Stratification factors include the TKI
choice (sunitinib vs cabozantinib) and IMDC prognostic