istration three times a day, intravenously or intraperitoneally
from 4 to 21 days in a single course. Three of six
patients with metastatic melanoma experienced a partial
response with >50% decrease in tumor volume. There was
no response to treatment in the other four patients with
colorectal or ovarian cancer. Marked lymphocytic infiltrate
was noted in a patient with lesions accessible to repeated
biopsies. This study was the first in human
evidence that the administration of IL-2 could mediate
the regression of cancer in some patients.15 Outside of
this phase I trial a single patient with renal cell carcinoma
with lung metastasis treated with IL-2 demonstrated a
complete response.15
Following this promising result, in a phase 2 study,
283 patients with metastatic melanoma and RCC were
treated with IL-2 at a dose of 720,000 IU/kg intravenously
every 8 hours for a maximum of 15 doses per cycle; a 7%
complete response and 10-13% partial response was observed
in each subgroup. Three patients had treatmentrelated
death. The major adverse event in these early
studies was fever, chills, GI symptoms, weight gain, pulmonary
edema, hypotension secondary to capillary leak
syndrome.16 Based on responses in phase 1 and phase 2
trials, the FDA approved high-dose IL-2, Aldesleukin in
RCC in 1992 and metastatic melanoma in 1998.17 However,
due to the severe toxicity profile, only specialized
centers were allowed to use high dose IL-2 immunotherapy.
Interleukin 2, IL-2 Receptor and Biology
Interleukin 2 gene, located on human chromosome 4, is
heavily regulated with several transcription factors, including
NF-kB, NF-AT and AP1 that are the downstream
products of signaling pathways activated with TCR/CD3
trigger and CD28 costimulation on CD4+, CD8+ Tcells.
18,19 It is also secreted by NK, NK-T cells, DCs and
mast cells following activation.20 The initial product of
the gene is 153 amino acids protein, processed with the
cleavage of 20 amino acid hydrophobic leader sequence
20 Kidney Cancer Journal
and O-linked glycosylation
of threonine 3, important in
cellular trafficking.21 It has
Type I cytokine structure with
4 alpha helical bundles
linked with a disulfide bond
between cysteines 58 and
105.10 The IL-2 receptor has
three non-covalently linked
components called IL-2Ra
(CD25, p55), IL-2Rb (CD122,
p75) and IL-2Rg (CD132,
p65). The IL-2 is able to bind
monomeric IL-2Ra , dimeric
IL-2Rbg and trimeric IL-
2Rabg forms of the receptor
with low-, intermediate-, and
high-affinity, respectively.22,23
Different immune cells express
the receptor at different
levels, either at resting or
with stimulation. This provides
diverse effects on immune
cells. In one end, it suppresses the immune
response through Tregs, which express CD25 constitutively
along with other subunits and have a high affinity
to IL-2 (Figure 2). On the other end, it provides effector
functions through Teff and NK cells. CD8+ and NK cells
tend to express the intermediate affinity receptor, IL-2Rbg.
Activated T-cells transiently express CD25 to enhance
their differentiation and proliferation as a response to IL-
2. IL-2 activates mainly JAK-STAT, RAS-MAP and PI3KAKT
pathways to induce proliferation and effector
functions of the immune cells.20,24 While PTEN, PD-1
and CTLA-4 inhibit PI3K-AKT pathway in Tregs, IL-2 also
activates Mst1-Mst2 which amplifies STAT5 and maintains
IL-2 induced Treg survival and stability.25
Strategies to Modulate IL-2
During the early studies, the major limitations of IL-2
therapy were high toxicity with capillary leak syndrome,
short half-life (15–30 min) and the requirement for highdose
to have adequate efficacy. Recent studies showed
that limiting toxicity, including capillary leak syndrome
and pulmonary edema, was mediated by CD25 stimulation
of pulmonary endothelial cells.26 Along with that,
the strategies described below investigated new formulations
of IL-2 that will prefer binding to CD122 and limit
CD25 based stimulation on Tregs to improve both toxicity
and efficacy profile (Figure 3). RG7461 (RO6874281)
is a recombinant fusion protein comprised of an engineered
form of IL-2 (IL-2v), carrying the mutations F42A,
Y45A and L72G. It is located in the CD25-binding epitope
of IL-2 and a human monoclonal antibody directed
against fibroblast activation protein-alpha (FAP) which is
strongly expressed on tumor-associated fibroblasts.27.28
Upon administration of RG7461, the monoclonal antibody
recognizes FAB and mediates retention and accumulation
of IL-2v in malignant lesions. Due to the
mutations on the CD25-binding epitope, IL-2v cannot
bind to CD25 and does not activate Tregs. IL-2v maintains
the ability to stimulate local immune response and acti-
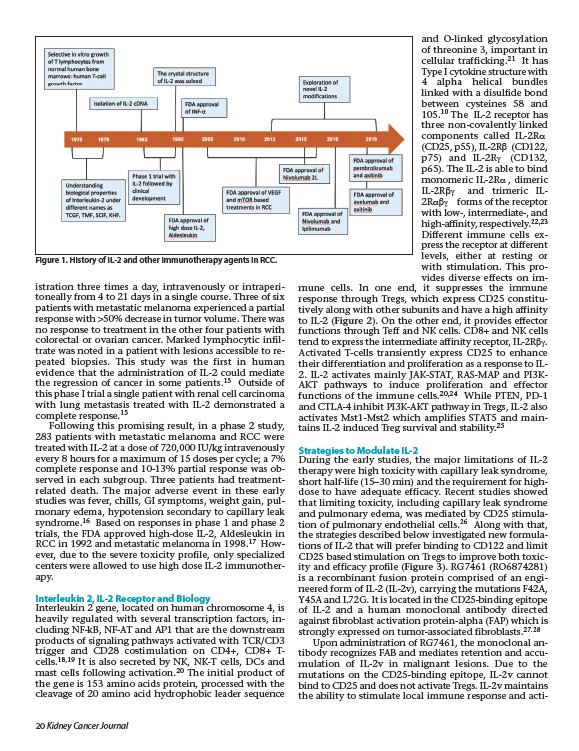
Figure 1. History of IL-2 and other immunotherapy agents in RCC.