To further develop a treatment plan, digital impressions and
bite registration were captured using the CS 3600 (Carestream
Dental) intraoral scanner (Figure 2 & 3). In addition
to illustrating the current condition to the patient during her
case presentation, the digital images were used for further
analysis of tooth position, tooth size and arch form for the
proposed treatment of full mouth edentulation, leveling and
grafting. Immediate dentures for both arches would be delivered
on the day of surgery, however in the lower arch four
dental implants would be placed to support an overdenture.
Financing options using a third party payment option (Lending
Club) were discussed with the patient. This discussion
was a very important part of facilitating acceptance of her
care, since it made the cost of treatment more feasible.
Starting in the maxillary arch, the teeth were extracted using
the Physics Forceps (Goldendent). The Physics Forceps act
simply like a class I lever, where only one force is applied
with the beak on the lingual aspect of the tooth. Once the
beak is placed at the lingual cervical portion, the soft bumper
is placed on the buccal alveolar ridge at the approximate
location of the muco-gingival junction to balance the beak.
The beak grasps the tooth, while the bumper is the fulcrum
to provide leverage and stability for the beak. Extraction is
accomplished with wrist movement rotation in a buccal direction
which is usually accomplished within 30-60 seconds
depending on the tooth morphology.
Once the teeth in the maxillary arch were removed, any granulation
tissue remaining within the sockets were removed
using a curette and any sharp areas of the alveolar crest were
leveled with a bone bur (Goldendent) and smoothed with a
��������������������������������������������������������������������
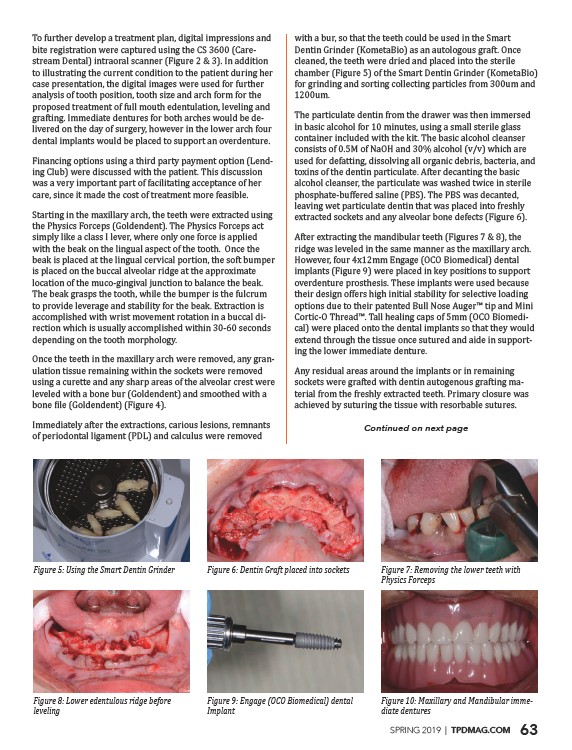
Immediately after the extractions, carious lesions, remnants
of periodontal ligament (PDL) and calculus were removed
with a bur, so that the teeth could be used in the Smart
Dentin Grinder (KometaBio) as an autologous graft. Once
cleaned, the teeth were dried and placed into the sterile
chamber (Figure 5) of the Smart Dentin Grinder (KometaBio)
for grinding and sorting collecting particles from 300um and
1200um.
The particulate dentin from the drawer was then immersed
in basic alcohol for 10 minutes, using a small sterile glass
container included with the kit. The basic alcohol cleanser
consists of 0.5M of NaOH and 30% alcohol (v/v) which are
used for defatting, dissolving all organic debris, bacteria, and
toxins of the dentin particulate. After decanting the basic
alcohol cleanser, the particulate was washed twice in sterile
phosphate-buffered saline (PBS). The PBS was decanted,
leaving wet particulate dentin that was placed into freshly
extracted sockets and any alveolar bone defects (Figure 6).
After extracting the mandibular teeth (Figures 7 & 8), the
ridge was leveled in the same manner as the maxillary arch.
However, four 4x12mm Engage (OCO Biomedical) dental
implants (Figure 9) were placed in key positions to support
overdenture prosthesis. These implants were used because
their design offers high initial stability for selective loading
������������������������������������������������������������������������������������������������������������������������
��������������������������������������������������������������������������������������������������������������-
cal) were placed onto the dental implants so that they would
extend through the tissue once sutured and aide in supporting
the lower immediate denture.
Any residual areas around the implants or in remaining
sockets were grafted with dentin autogenous grafting material
from the freshly extracted teeth. Primary closure was
achieved by suturing the tissue with resorbable sutures.
Continued on next page
���������������������������������������������������������������������������������� �������������������������������������������������������������������������������������� ��������������������������������������������������������������������������������
������������������������������
��������������������������������������������������������������������������������
������������������
����������������������������������������������������������������������������������
����������������
��������������������������������������������������������������������������������-
��������������������������������
SPRING 2019 | TPDMAG.COM 63
/TPDMAG.COM