��������������������������������������������������������������
������������������������������������������������������������������������
Reduction Strategies - Part 1 of 4
(Continued from page 57)
pick up material. Petroleum jelly was applied to the surrounding
surfaces of the denture to prevent unwanted
adherence of excess material. Once mixed, the Tokuyama
Rebase II material (Figure 15 & 16) was placed into a plastic
dispensing syringe and injected up to two thirds the height of
each recess as well as on to the attachments. During seating,
the prosthesis was gently held in place by hand. After a total
of about 3 minutes, the overdenture with the incorporated
retention caps was removed. Any excess material was
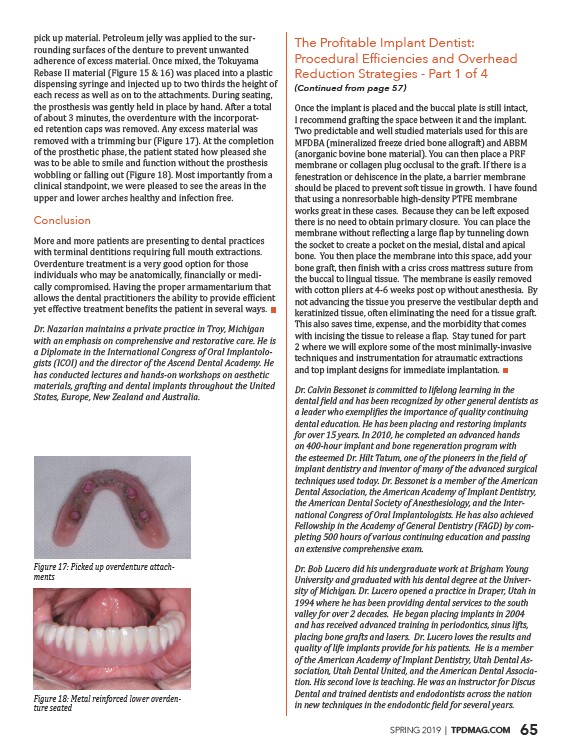
removed with a trimming bur (Figure 17). At the completion
of the prosthetic phase, the patient stated how pleased she
was to be able to smile and function without the prosthesis
wobbling or falling out (Figure 18). Most importantly from a
clinical standpoint, we were pleased to see the areas in the
upper and lower arches healthy and infection free.
Conclusion
More and more patients are presenting to dental practices
with terminal dentitions requiring full mouth extractions.
Overdenture treatment is a very good option for those
����������������������������������������������������������������������������������������������������������������-
cally compromised. Having the proper armamentarium that
����������������������������������������������������������������������������������������������������������������������������������
������������������������������������������������������������������������������������������������������������������������������
������������������������������������������������������������������������������������������������������������������������
����������������������������������������������������������������������������������������������������������������������������
������������������������������������������������������������������������������������������������������������������������-
������������������������������������������������������������������������������������������������������������������������������
����������������������������������������������������������������������������������������������������������������������
����������������������������������������������������������������������������������������������������������������������������
��������������������������������������������������������������������������������������
������������������������������������������������������������������������������-
��������������
����������������������������������������������������������������������������������-
����������������������
Once the implant is placed and the buccal plate is still intact,
I recommend grafting the space between it and the implant.
Two predictable and well studied materials used for this are
MFDBA (mineralized freeze dried bone allograft) and ABBM
(anorganic bovine bone material). You can then place a PRF
membrane or collagen plug occlusal to the graft. If there is a
fenestration or dehiscence in the plate, a barrier membrane
should be placed to prevent soft tissue in growth. I have found
that using a nonresorbable high-density PTFE membrane
works great in these cases. Because they can be left exposed
there is no need to obtain primary closure. You can place the
����������������������������������������������������������������������������������������������������������������������
the socket to create a pocket on the mesial, distal and apical
bone. You then place the membrane into this space, add your
��������������������������������������������������������������������������������������������������������������������������������
the buccal to lingual tissue. The membrane is easily removed
with cotton pliers at 4-6 weeks post op without anesthesia. By
not advancing the tissue you preserve the vestibular depth and
keratinized tissue, often eliminating the need for a tissue graft.
This also saves time, expense, and the morbidity that comes
����������������������������������������������������������������������������������������������������������������������������������
2 where we will explore some of the most minimally-invasive
techniques and instrumentation for atraumatic extractions
and top implant designs for immediate implantation.
��������������������������������������������������������������������������������������������������������������������������
������������������������������������������������������������������������������������������������������������������������������������
����������������������������������������������������������������������������������������������������������������������������
��������������������������������������������������������������������������������������������������������������������������
����������������������������������������������������������������������������������������������������������������������
��������������������������������������������������������������������������������������������������������������
����������������������������������������������������������������������������������������������������������������������������������
��������������������������������������������������������������������������������������������������������������������������������
��������������������������������������������������������������������������������������������������������������������������������
������������������������������������������������������������������������������������������������������������������������������
������������������������������������������������������������������������������������������������������������������������-
��������������������������������������������������������������������������������������������������������������������������������
������������������������������������������������������������������������������������������������������������������������-
����������������������������������������������������������������������������������������������������������������������������
����������������������������������������������������������������
����������������������������������������������������������������������������������������������������������������������
��������������������������������������������������������������������������������������������������������������������������-
������������������������������������������������������������������������������������������������������������������������������������
����������������������������������������������������������������������������������������������������������������������������
����������������������������������������������������������������������������������������������������������������������������
����������������������������������������������������������������������������������������������������������������������������������
������������������������������������������������������������������������������������������������������������������������������������
��������������������������������������������������������������������������������������������������������������������������������������
������������������������������������������������������������������������������������������������������������������������-
����������������������������������������������������������������������������������������������������������������������������-
��������������������������������������������������������������������������������������������������������������������������������������
������������������������������������������������������������������������������������������������������������������������������
������������������������������������������������������������������������������������������������������������������������
SPRING 2019 | TPDMAG.COM 65
/TPDMAG.COM