The more critical patient will need to go to the ICU. In the
ICU, they will want to monitor the pressure in the brain; if the
pressure in the brain goes up this can cause further damage. To
monitor the pressure (called cerebral perfusion pressure), the
doctors will place a small tube in the brain. This tube is called an
intra-ventricular catheter or sometimes an intra-cerebral pressure
(ICP) catheter. The ICP catheter is inserted by drilling a hole
in the skull and inserting the tube into the brain. This tube will
allow the doctors and nurses to monitor the pressure inside the
brain and drain off extra fluid (cerebral spinal fluid) if needed. If
the pressure in the brain remains high, then medications can be
given to help decrease the swelling of the brain. Sometimes, if the
swelling can’t be stopped the patient may need to go immediately
to the operating room.
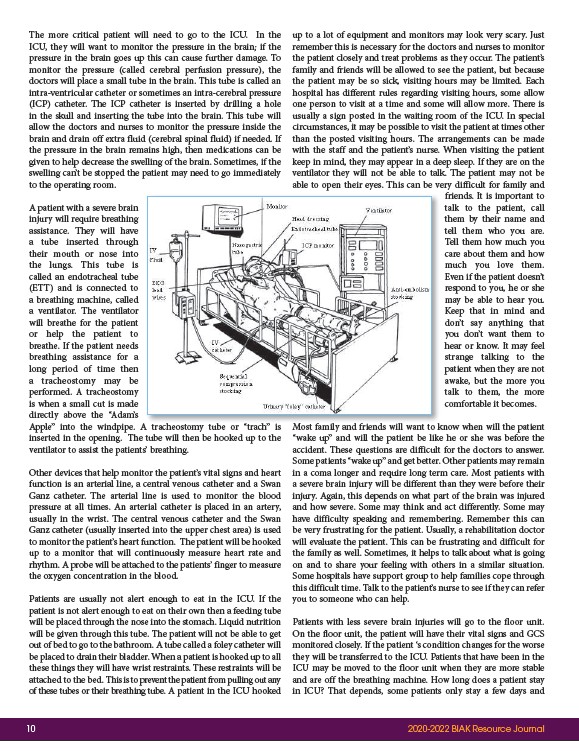
A patient with a severe brain
injury will require breathing
assistance. They will have
a tube inserted through
their mouth or nose into
the lungs. This tube is
called an endotracheal tube
(ETT) and is connected to
a breathing machine, called
a ventilator. The ventilator
will breathe for the patient
or help the patient to
breathe. If the patient needs
breathing assistance for a
long period of time then
a tracheostomy may be
performed. A tracheostomy
is when a small cut is made
directly above the “Adam’s
Apple” into the windpipe. A tracheostomy tube or trach” is
inserted in the opening. The tube will then be hooked up to the
ventilator to assist the patients’ breathing.
Other devices that help monitor the patient’s vital signs and heart
function is an arterial line, a central venous catheter and a Swan
Ganz catheter. The arterial line is used to monitor the blood
pressure at all times. An arterial catheter is placed in an artery,
usually in the wrist. The central venous catheter and the Swan
Ganz catheter (usually inserted into the upper chest area) is used
to monitor the patient’s heart function. The patient will be hooked
up to a monitor that will continuously measure heart rate and
rhythm. A probe will be attached to the patients’ finger to measure
the oxygen concentration in the blood.
Patients are usually not alert enough to eat in the ICU. If the
patient is not alert enough to eat on their own then a feeding tube
will be placed through the nose into the stomach. Liquid nutrition
will be given through this tube. The patient will not be able to get
out of bed to go to the bathroom. A tube called a foley catheter will
be placed to drain their bladder. When a patient is hooked up to all
these things they will have wrist restraints. These restraints will be
attached to the bed. This is to prevent the patient from pulling out any
of these tubes or their breathing tube. A patient in the ICU hooked
up to a lot of equipment and monitors may look very scary. Just
remember this is necessary for the doctors and nurses to monitor
the patient closely and treat problems as they occur. The patient’s
family and friends will be allowed to see the patient, but because
the patient may be so sick, visiting hours may be limited. Each
hospital has different rules regarding visiting hours, some allow
one person to visit at a time and some will allow more. There is
usually a sign posted in the waiting room of the ICU. In special
circumstances, it may be possible to visit the patient at times other
than the posted visiting hours. The arrangements can be made
with the staff and the patient’s nurse. When visiting the patient
keep in mind, they may appear in a deep sleep. If they are on the
ventilator they will not be able to talk. The patient may not be
able to open their eyes. This can be very difficult for family and
friends. It is important to
talk to the patient, call
them by their name and
tell them who you are.
Tell them how much you
care about them and how
much you love them.
Even if the patient doesn’t
respond to you, he or she
may be able to hear you.
Keep that in mind and
don’t say anything that
you don’t want them to
hear or know. It may feel
strange talking to the
patient when they are not
awake, but the more you
talk to them, the more
comfortable it becomes.
A h b “ h”i M f il d f i d ill k
Most family and friends will want to know when will the patient
“wake up” and will the patient be like he or she was before the
accident. These questions are difficult for the doctors to answer.
Some patients “wake up” and get better. Other patients may remain
in a coma longer and require long term care. Most patients with
a severe brain injury will be different than they were before their
injury. Again, this depends on what part of the brain was injured
and how severe. Some may think and act differently. Some may
have difficulty speaking and remembering. Remember this can
be very frustrating for the patient. Usually, a rehabilitation doctor
will evaluate the patient. This can be frustrating and difficult for
the family as well. Sometimes, it helps to talk about what is going
on and to share your feeling with others in a similar situation.
Some hospitals have support group to help families cope through
this difficult time. Talk to the patient’s nurse to see if they can refer
you to someone who can help.
Patients with less severe brain injuries will go to the floor unit.
On the floor unit, the patient will have their vital signs and GCS
monitored closely. If the patient ‘s condition changes for the worse
they will be transferred to the ICU. Patients that have been in the
ICU may be moved to the floor unit when they are more stable
and are off the breathing machine. How long does a patient stay
in ICU? That depends, some patients only stay a few days and
10 2020-2022 BIAK Resource Journal